Articles
- Page Path
- HOME > Epidemiol Health > Volume 44; 2022 > Article
-
Methods
The clinical meaning of the area under a receiver operating characteristic curve for the evaluation of the performance of disease markers -
Stefano Parodi1
 , Damiano Verda2, Francesca Bagnasco1, Marco Muselli2,3
, Damiano Verda2, Francesca Bagnasco1, Marco Muselli2,3 -
Epidemiol Health 2022;44:e2022088.
DOI: https://doi.org/10.4178/epih.e2022088
Published online: October 17, 2022
1Scientific Directorate, IRCCS Istituto Giannina Gaslini, Genoa, Italy
2Rulex Innovation Labs, Genoa, Italy
3Institute of Electronics, Computer and Telecommunication Engineering, National Research Council of Italy, Genoa, Italy
- Correspondence: Stefano Parodi, Scientific Directorate, IRCCS Istituto Giannina Gaslini, Largo G. Gaslini 5, Genoa 16147, Italy, E-mail: parodistefano@icloud.com
© 2022, Korean Society of Epidemiology
This is an open-access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
OBJECTIVES
- The area under a receiver operating characteristic (ROC) curve (AUC) is a popular measure of pure diagnostic accuracy that is independent from the proportion of diseased subjects in the analysed sample. However, its actual usefulness in the clinical context has been questioned, because it does not seem to be directly related to the actual performance of a diagnostic marker in identifying diseased and non-diseased subjects in real clinical settings. This study evaluates the relationship between the AUC and the proportion of correct classifications (global diagnostic accuracy, GDA) in relation to the shape of the corresponding ROC curves.
-
METHODS
- We demonstrate that AUC represents an upward-biased measure of GDA at an optimal accuracy cut-off for balanced groups. The magnitude of bias depends on the shape of the ROC plot and on the proportion of diseased and non-diseased subjects. In proper curves, the bias is independent from the diseased/non-diseased ratio and can be easily estimated and removed. Moreover, a comparison between 2 partial AUCs can be replaced by a more powerful test for the corresponding whole AUCs.
-
RESULTS
- Applications to 3 real datasets are provided: a marker for a hormone deficit in children, 2 tumour markers for malignant mesothelioma, and 2 gene expression profiles in ovarian cancer patients.
-
CONCLUSIONS
- The AUC is a measure of accuracy with potential clinical relevance for the evaluation of disease markers. The clinical meaning of ROC parameters should always be evaluated with an analysis of the shape of the corresponding ROC curve.
- Receiver operating characteristic (ROC) curves are standard statistical tools for the analysis of disease markers (DMs). The area under a ROC curve (AUC) is a popular measure of diagnostic accuracy that represents an estimator of the probability of correctly ranking a pair of subjects: one extracted from the class of diseased individuals and the other from that of non-diseased individuals [1].
- Despite its popularity, the actual usefulness and the meaning of the AUC in clinical settings have been intensely questioned. One of the major criticisms is that patients are not presented to physicians in diseased/non-diseased pairs; thus, the clinical meaning of the AUC remains unclear [2–5]. Furthermore, the AUC is an average measure of sensitivity calculated over the complete set of specificity values, including those with poor clinical relevance. For this reason, in many instances the partial area (pAUC) is preferred to the AUC. The pAUC can be computed in a range of specificity or sensitivity values that are deemed meaningful [6,7]. In most cases, the pAUC is calculated between 0 and the highest acceptable false positive rate, and the performance of 2 DMs is evaluated by comparing the 2 corresponding pAUCs [3,8,9]. However, such a comparison may be prone to insufficient statistical power, the results of the test can strongly depend on the selected range of specificity, and the estimation of the pAUC is likely to be more noticeably affected than that of the AUC by the shape of the fitted ROC curve [10,11].
- In the next paragraphs, we briefly review the principles of ROC analysis. We show that the AUC represents an optimistic (i.e., upward-biased) estimate of the proportion of subjects that could be correctly classified by a binary test in the presence of balanced groups (the same proportion of diseased and non-diseased patients). We demonstrate that the relationship between AUC and global accuracy is independent from the proportion of diseased subjects when the curve has a regular shape (a proper ROC curve). Finally, we demonstrate that, under a proper model, 2 pAUCs can be compared by a more powerful test for the corresponding AUCs. For illustration, we present applications to 3 real datasets for the evaluation of the diagnostic accuracy of different DMs.
- The R scripts [12] developed ad hoc for the present study are listed in the Supplementary Material 1 with an example of their application.
INTRODUCTION
- Principles of receiver operating characteristic analysis
- The early steps for marker validation, in general, require a case-control approach; therefore, following a widespread convention, in this article the class of diseased subjects will be referred to as “cases” and the referent group as “controls” [13].
- Given a continuous DM, a binary diagnostic test can be defined selecting a cut-off value c and classifying as test-positive any DM value >c. The probability of a correct classification among cases is called sensitivity, Se(c) (also referred to as the true-positive rate), and that among controls is referred to as specificity, Sp(c) (the false-positive rate). An empirical ROC curve is obtained by plotting each Se(c) vs. the corresponding 1-Sp(c) for any observed c [8].
- The global diagnostic accuracy (GDA) represents the probability of a correct classification at each cut-off c and is a linear function of Se(c) and Sp(c) [14]:
- where π represents the proportion of cases (often referred to as “disease prevalence”).
- Combining Se(c) and Sp(c), 2 measures of accuracy independent from π can be obtained (pure accuracy indices), namely, the Youden index (J):
- and the diagnostic odds ratio (DOR) [14]:
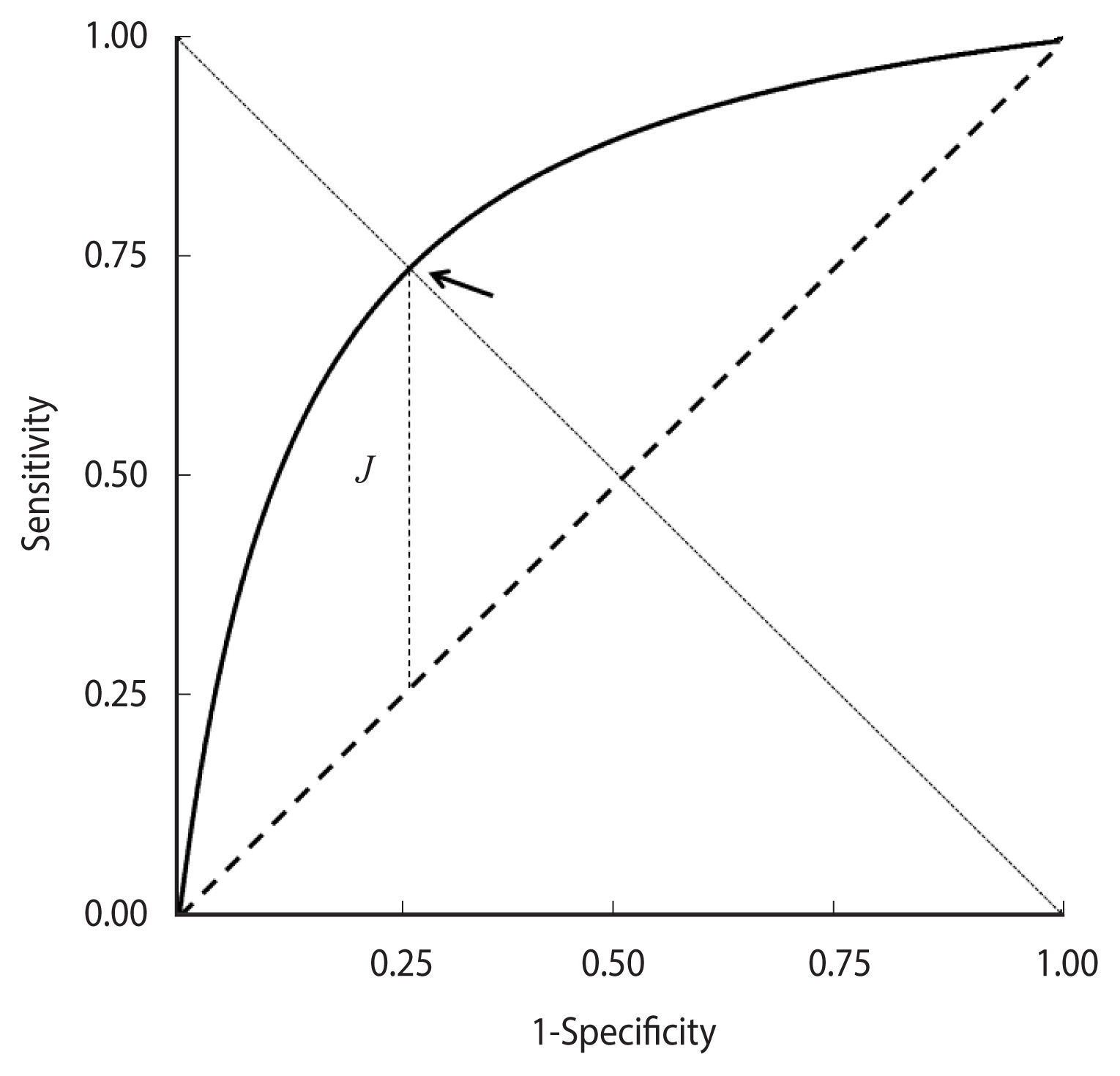
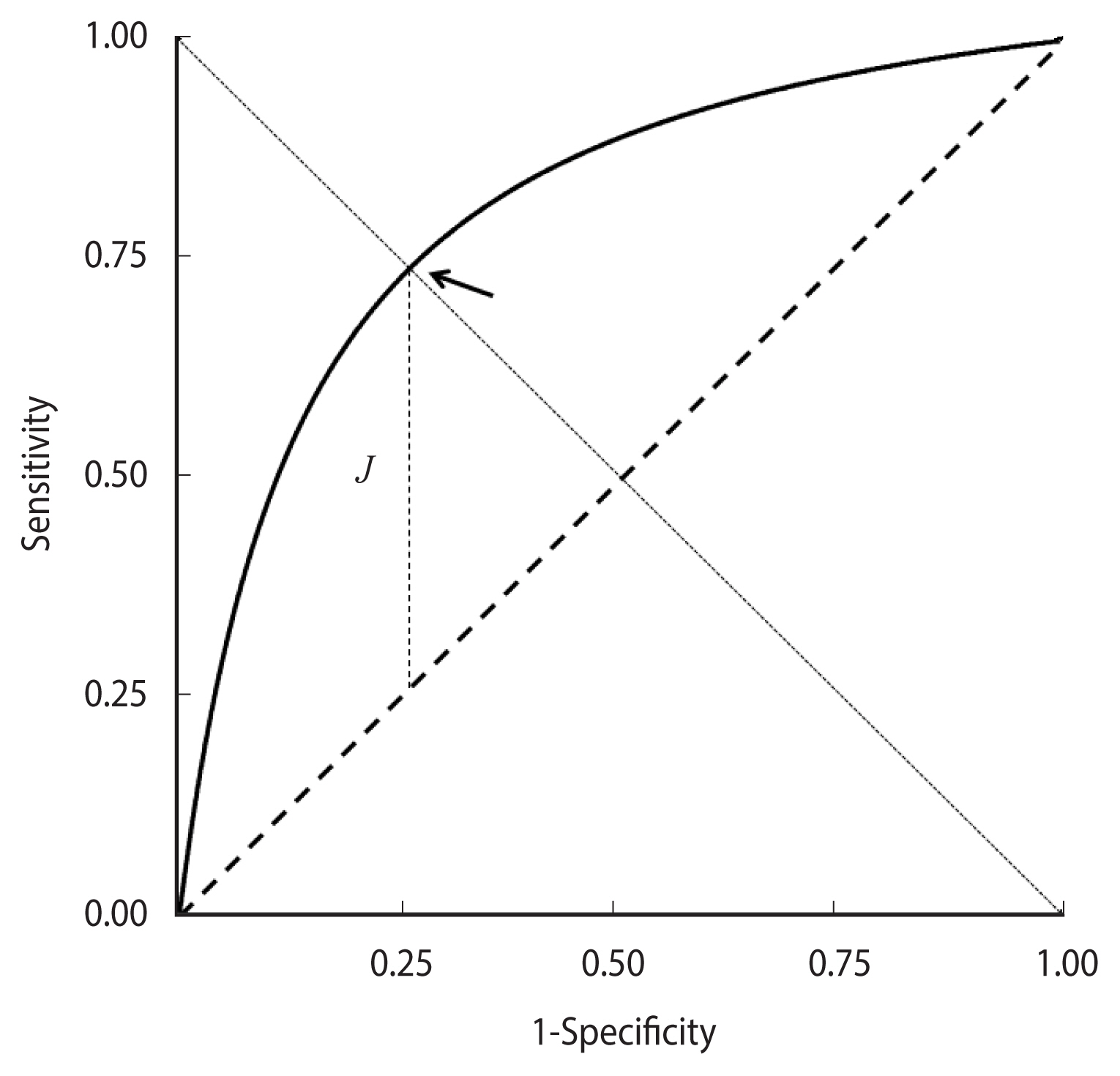
- J corresponds to the vertical distance of the ROC curve from the rising diagonal. Its maximum value, which equals the Kolmogorov-Smirnov test statistic, identifies an “optimal” cut-off that corresponds to the minimum value of the sum of false positive and false negative proportions [8].
- Replacing Se(c) with y and 1-Sp(c) with x in equation (3), the equation of a ROC curve is obtained as a function of DOR; in the case of a constant DOR, it becomes [15]:
- Equation (4) can also be obtained from a “proper” binormal model—that is, hypothesising that DM values follow a normal distribution with different means in cases and controls and equal variances. Accordingly, the corresponding graph is called a proper binormal ROC curve [15–18]. The curve is concave and symmetric with respect to the descending diagonal and the point of the highest Youden index J corresponds to equal values of Se(c) and Sp(c) (Figure 1).
- An empirical ROC curve is invariant with respect to any transformation of the corresponding DM values that does not alter their original ranks; then, in a very general framework, the standard binormal model can be assumed if the DM distribution in cases and controls is transformable into 2 normal distributions by a monotonic function [19]. The correspondence between equation (4) and the parametric binormal model allows the application of statistical methods to assess the shape of a ROC curve. For instance, the departure of an empirical ROC curve from the proper model can be evaluated by the test proposed by Metz & Kronman [18].
- The clinical meaning of the area under a receiver operating characteristic curve
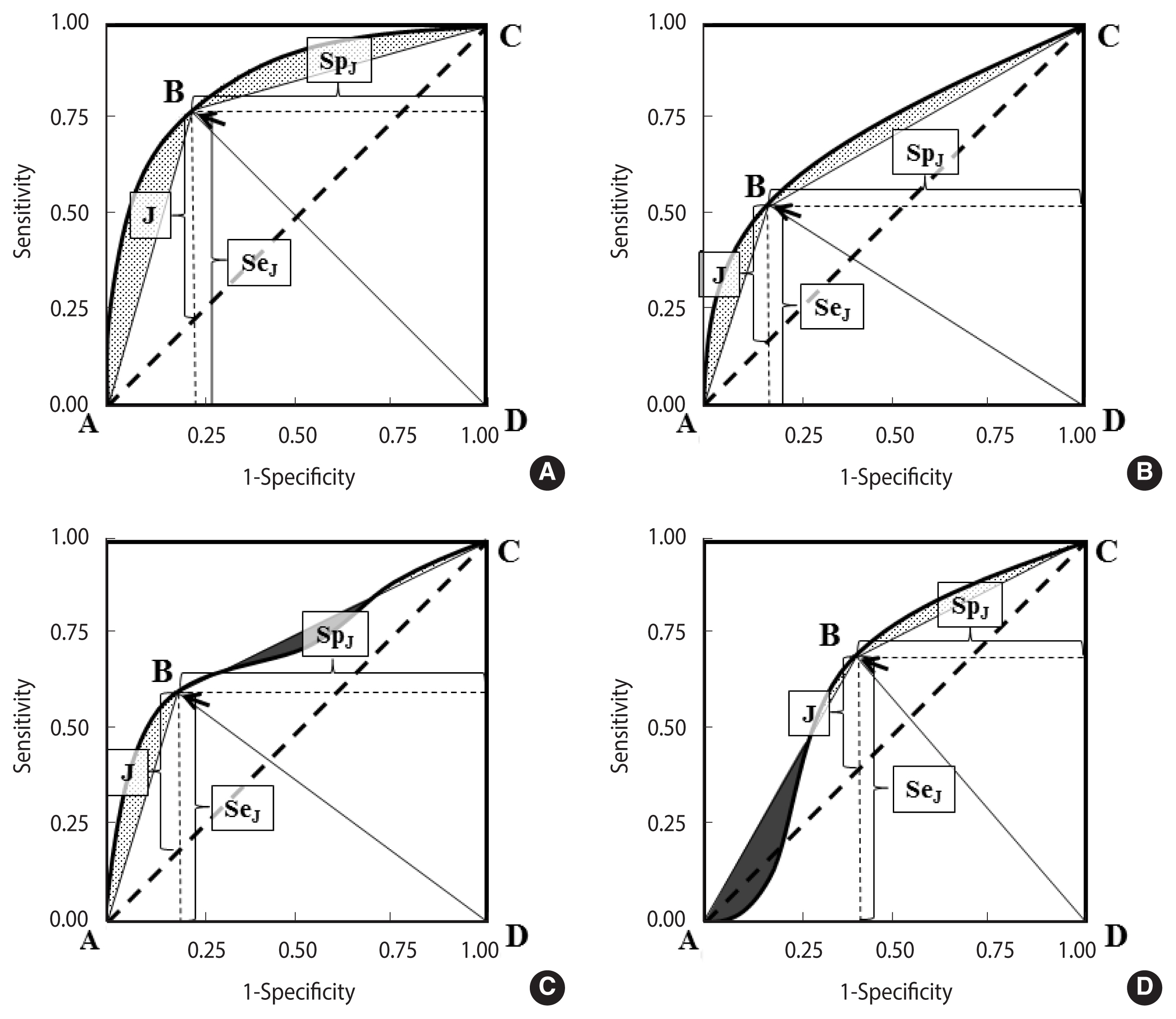
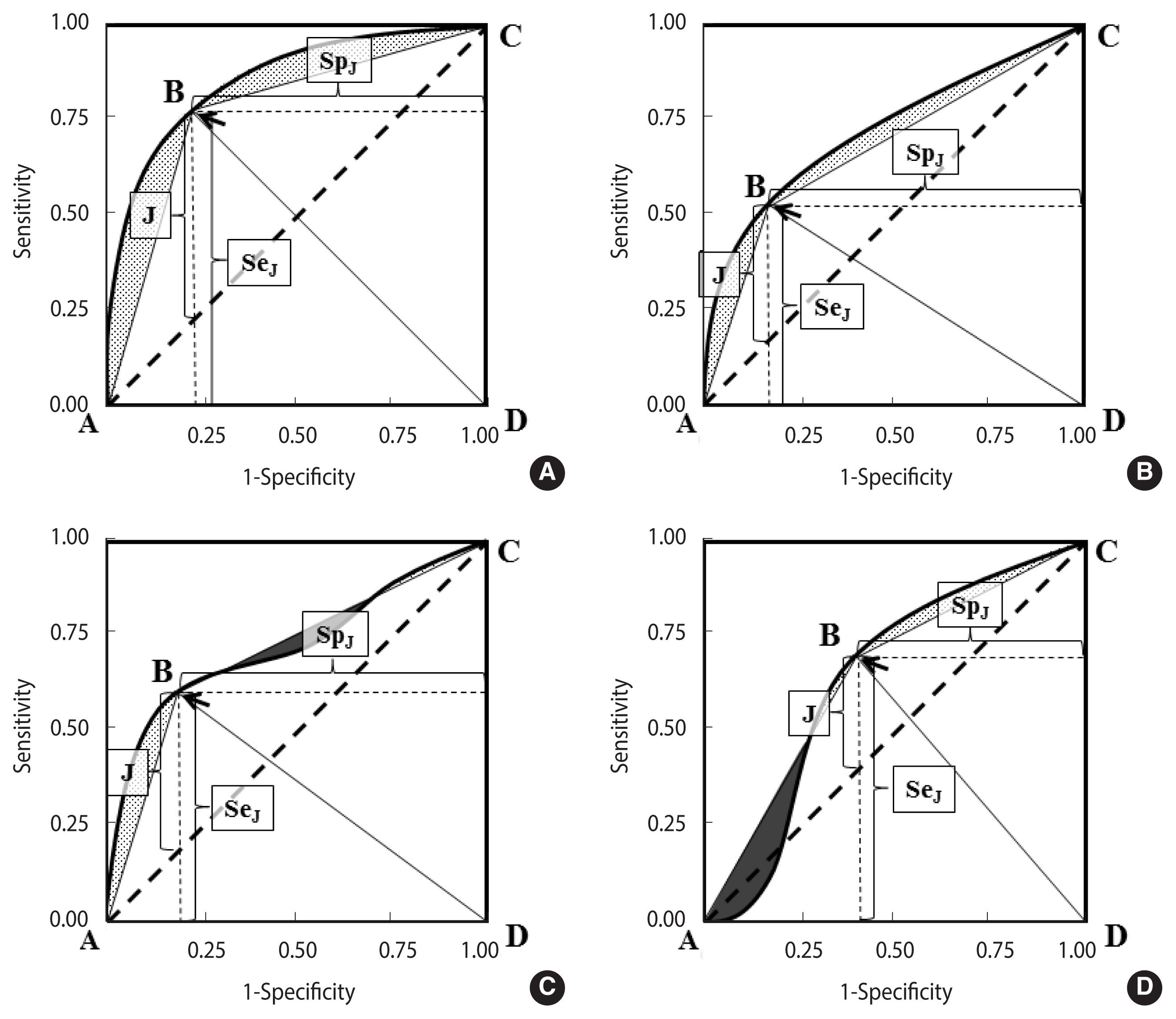
- Figure 2A–D shows 4 differently shaped ROC curves.
- In each curve, the optimal cut-off, corresponding to the highest Youden index (equation [2]), is indicated by an arrow.
- A polygon ABCD can be obtained by joining a point to the origin and to the upper right corner of the ROC plot. It can be noted that the area A of ABCD is a biased measure of the AUC:
- where b represents the “bias” that in concave curves corresponds to the area between the curve and the polygon (Figure 1, grey regions in panels A and B).
- The area delimited by ABCD is the sum of the areas under the 2 triangles ABD and BCD, whose bases are both equal to one and the heights are, respectively, the sensitivity and the specificity at the optimal cut-off:
- It can be noted that equation (5) is equivalent to equation (1) in the presence of a balanced sample (π=0.5), then:
- In a proper binormal theoretical ROC curve (Figure 2A), the optimal cut-off corresponds to the point of equal sensitivity and specificity; then, replacing SpJ with SeJ in equation (5), it is easy to verify that GDA no longer depends on π:
- In summary, the AUC represents an “optimistic” estimator of GDA; that is, it provides an upper bound for the proportion of correct classifications that can be obtained at an optimal accuracy cut-off and in the presence of 2 balanced groups. An interesting property of the proper binormal ROC curves is that the association between the AUC and GDA at the optimal cut-off is independent from the proportion of cases and controls.
- The amount of bias, b, depends on the shape of the ROC curve. A loss of concavity can reduce b, in part or completely (Figure 2, dark regions in panels C and D). Conversely, under a proper model (Figure 2A), b tends to be higher, but it can be calculated by applying the following equation:
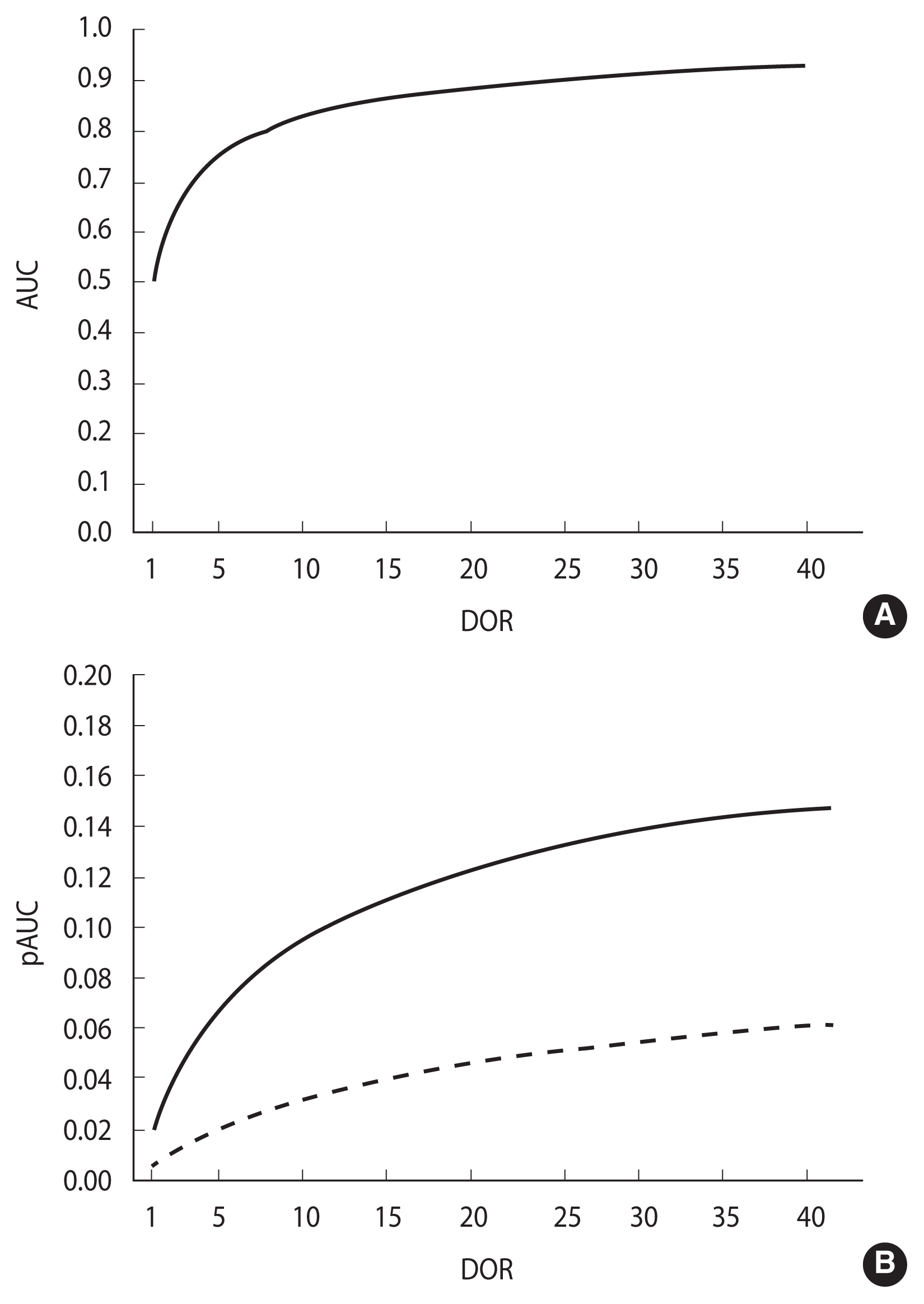
- as demonstrated in the Appendix 1. The DOR can be calculated from the corresponding AUC, using the following equation, obtained by integrating equation (4) [20]:
- A routine in R language (rocdor) is provided in the Supplementary Material 1 to calculate the DOR from the AUC via a numeric approach. The confidence intervals of the DOR can be estimated from equation (8) by replacing the AUC with the corresponding confidence intervals, obtained using the method of DeLong et al. [21].
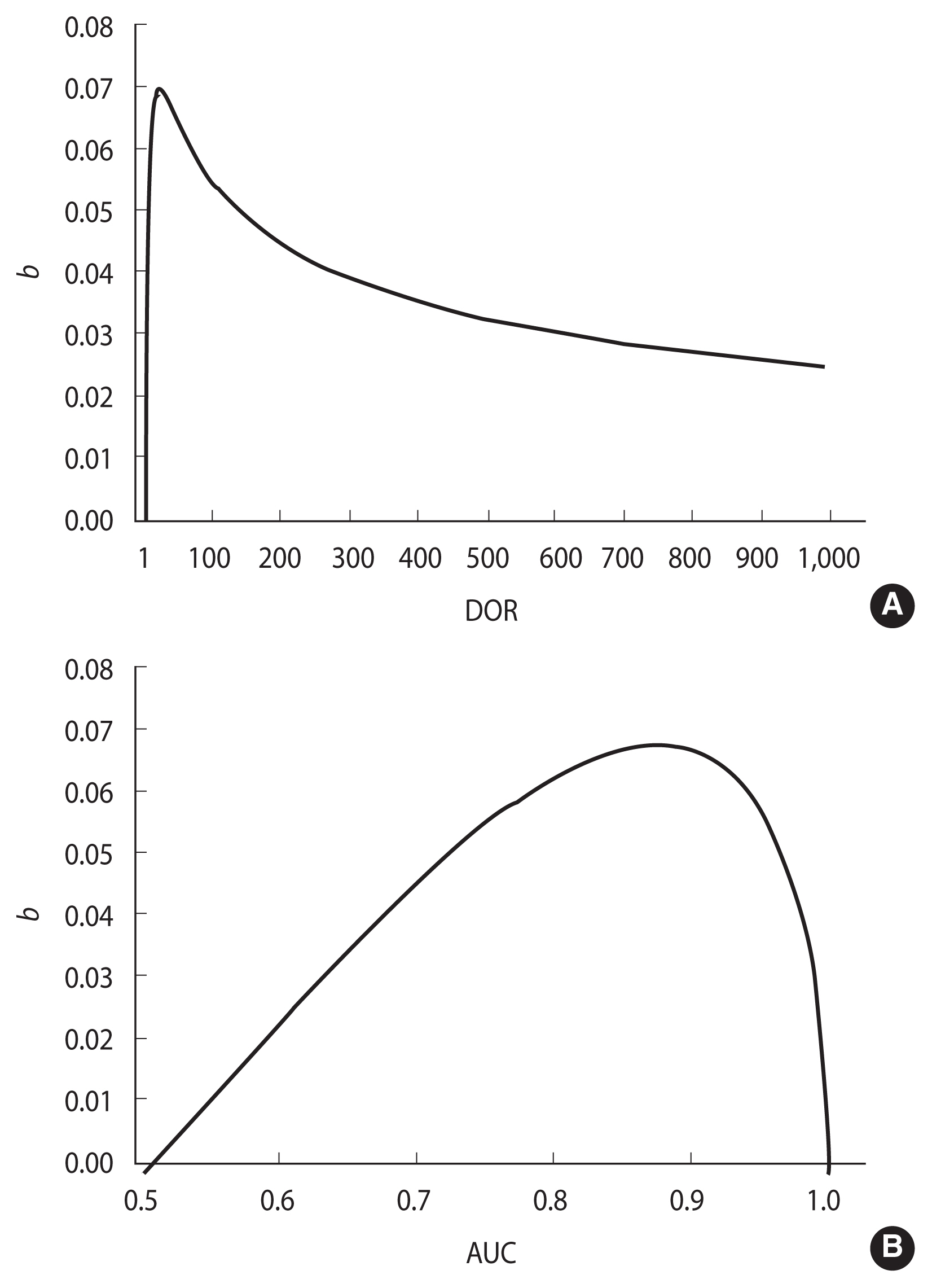
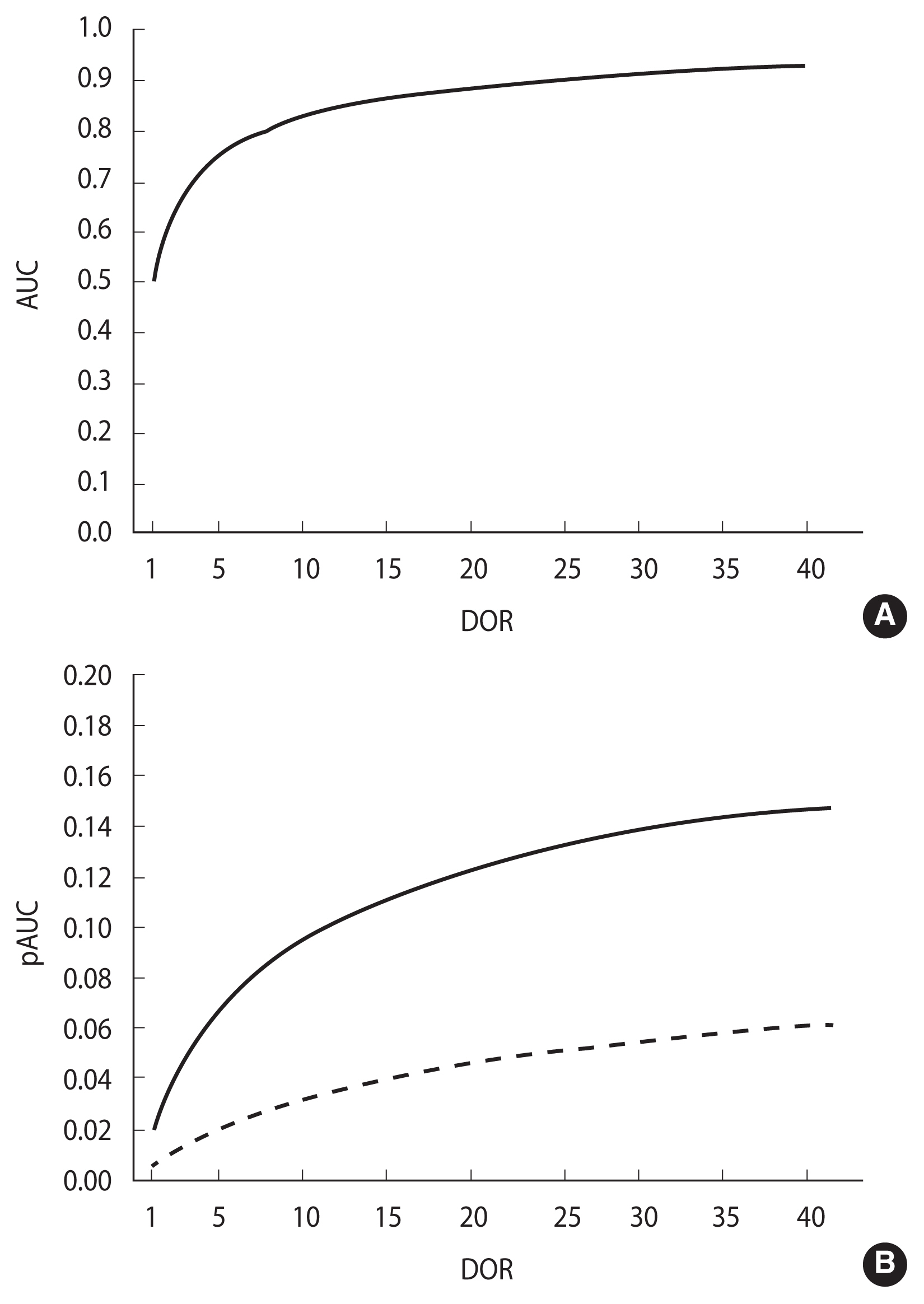
- Figure 3 shows the relationship between b and the DOR, according to equation (7) (Figure 3A) and between b and the AUC (Figure 3B). The highest b value (0.07) is observed for DOR=17.3, which corresponds to an AUC of 0.876. b tends toward 0 when the AUC is close to either 0.5 or 1.0. The first case corresponds to a DOR of 1.0 and to a non-informative ROC curve lying on the rising diagonal, while the latter corresponds to an infinite DOR and a perfect separation between DM values in cases and controls (Figure 3).
- Integrating equation (4) from 0 to k, k≤1, the association between the DOR and the partial area pAUC(k) between a specificity of k and 1.0 is obtained [22]:
- In a proper model, the association of both AUC and pAUC(k) with the DOR (equations (8) and (9), respectively) is monotonic and strictly increasing in the DOR, as depicted in Figure 4 (panels A and B, respectively). Accordingly, the inequalities AUC1>AUC2 and pAUC1>pAUC2 both imply and are implied by DOR1>DOR2. As a consequence, under a proper model assumption, the difference between 2 pAUCs can be assessed by testing the difference between the corresponding whole AUCs (Figure 4).
- The departure from a proper model of 2 empirical ROC curves can be checked by the Metz and Kronman test [18]. In the case of a significant result, a usual test for the comparison of 2 pAUCs can be employed. In this study, the bootstrap method by Robin et al. [9] was adopted and implemented by the authors in the pROC R library. Conversely, if the hypothesis of a proper model is not rejected, a standard test for the comparison of the corresponding AUCs is suggested to improve statistical power. In this investigation, we employed the method proposed by DeLong et al. [21].
- Data sets selected for the application to real data in diagnostic medical settings
- The first dataset (“GH deficit”) included 79 patients with a reversible growth hormone deficit (GHD) during childhood, as diagnosed by the insulin-tolerance test (ITT). The ITT measured at first diagnosis was eventually evaluated as a DM for permanent GHD during late adolescence. Permanent GHD was observed in 31 out of the 79 recruited patients [23].
- The second dataset (“malignant mesothelioma”) included 52 patients with malignant pleural mesothelioma and 117 patients affected by either benign pleurisies (n=55) or pleural metastases from other malignancies (n=62), and 2 tumour markers (namely, SMRP and Cyfra21-1) [24].
- The third dataset (“ovarian cancer”) included the expression of more than 1,500 genes in normal (n=23) and malignant (n=30) ovarian tissues [8]. In this study only the first 2 genes were analysed.
- The results of the application of the proposed approach of analysis are resumed in Supplementary Material 2 and illustrated in detail in the paragraphs below.
- Ethics statement
- Neither ethical committee approval nor informed consent were needed because the data analysed are publicly available on previously published papers and they are completely anonymized.
MATERIALS AND METHODS
The AUC is an estimator of GDA that depends on the shape of the ROC curve
Relationship between b and DOR
Relationship between the AUC, pAUC and DOR
Comparison between 2 ROC curves
- Area under the receiver operating characteristic (ROC) curve is an estimator of the global diagnostic accuracy at an optimal cut-off in a proper ROC curve
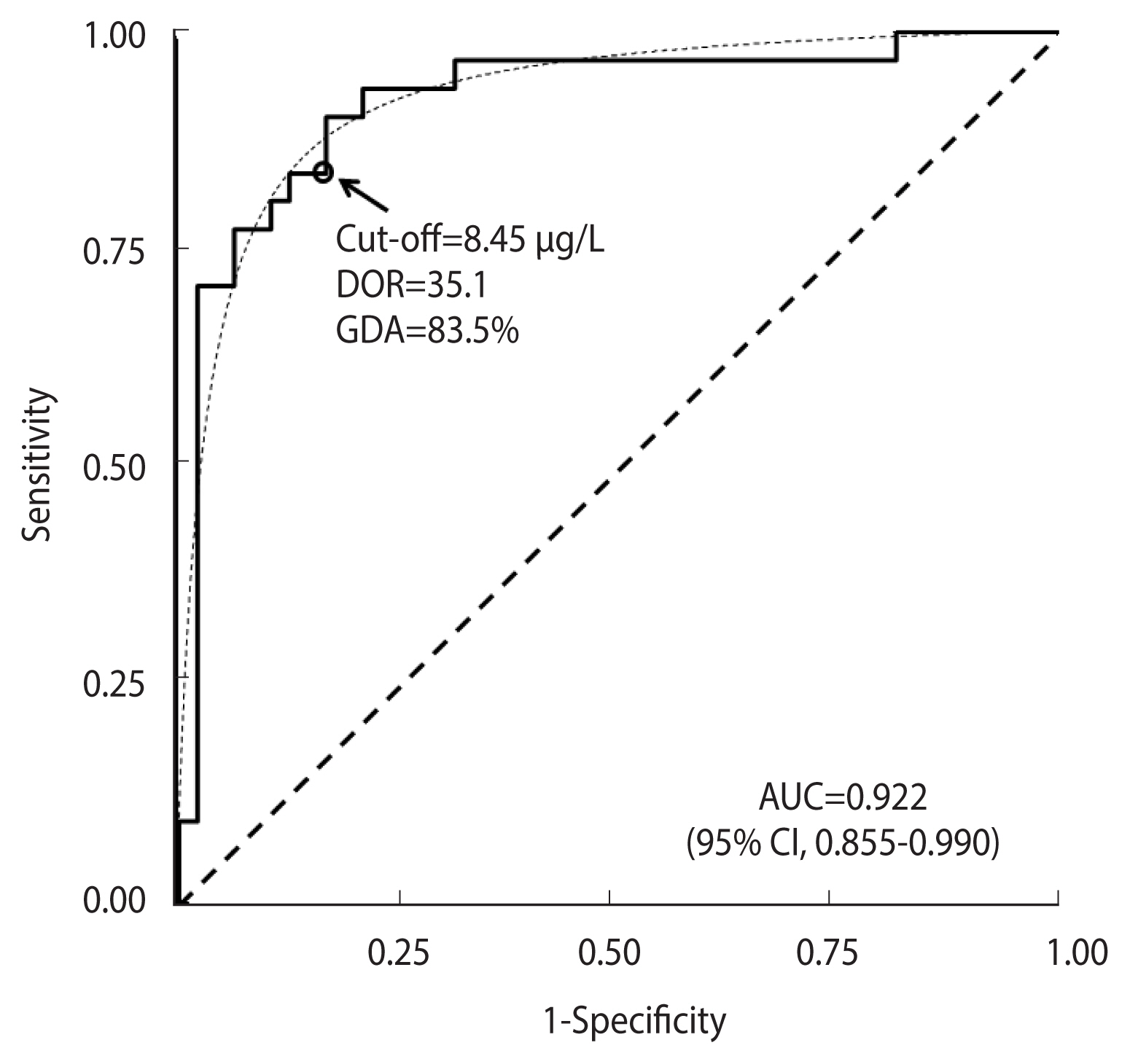
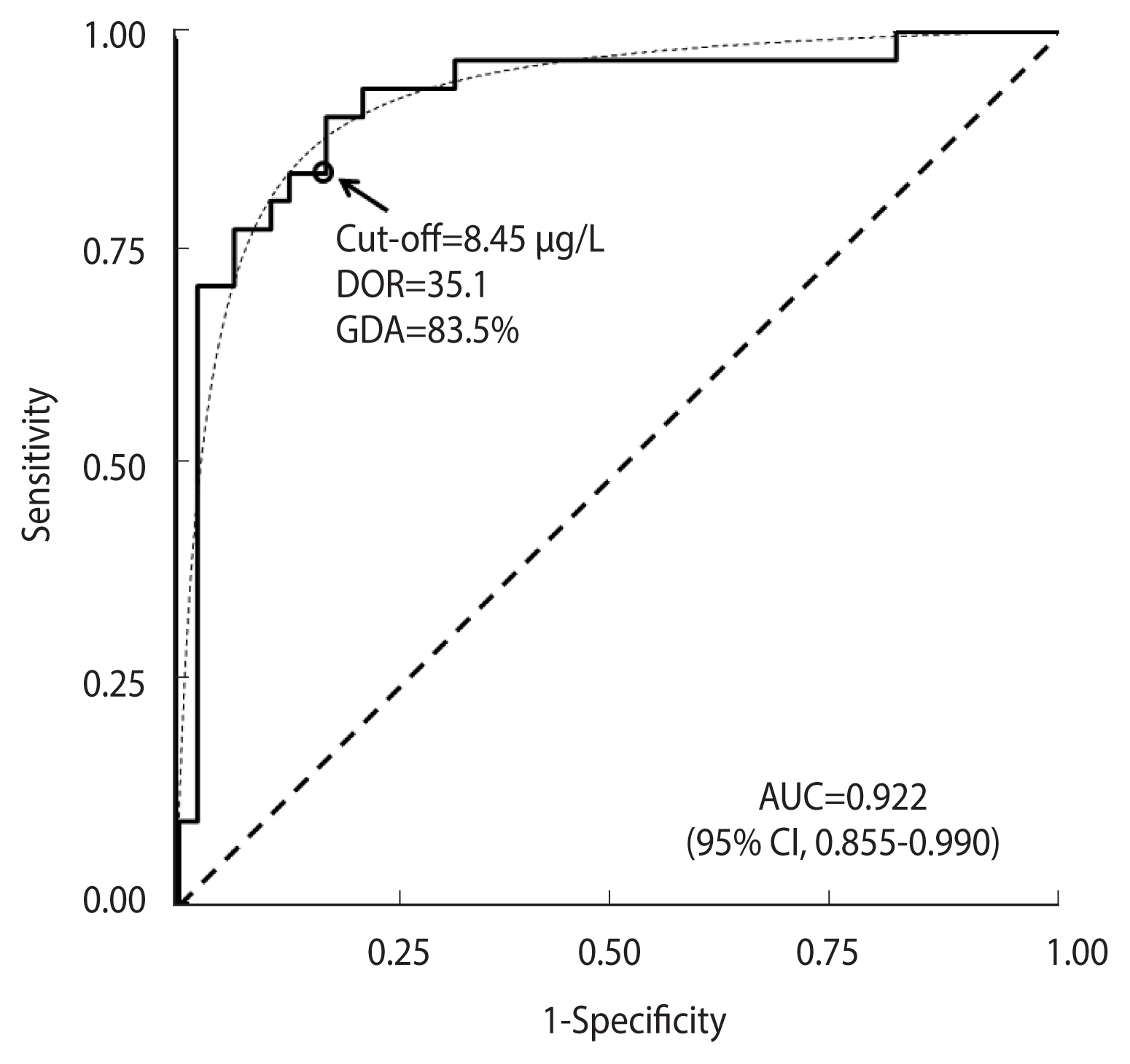
- Figure 5 shows the ROC curve obtained from the ITT test in the “GH deficit” dataset. The empirical estimate of AUC was 0.922 (95% CI, 0.855 to 0.990). The ROC curve fit the expected theoretical proper ROC very well (p=0.644, Metz and Kronman test). The corresponding DOR was 35.1. The cut-off of equal values for sensitivity and specificity corresponded to a DM value of 8.45 μg/L, as is indicated by a circle in Figure 5. The corresponding observed GDA was 83.5%.
- Applying equation (7), an estimate of the bias b of 0.066 (95% CI, 0.032 to 0.069) was obtained, which, subtracted from
- Comparison between a proper and a non-proper receiver operating characteristic curve
- Figure 6 shows a comparison between ROC curves corresponding to the distribution of the SMRP and Cyfra21-1 tumour markers in the “malignant mesothelioma” dataset.
- The AUC for SMRP was 0.842 (95% CI, 0.774 to 0.910), and that for Cyfra21-1 was 0.760 (95% CI, 0.687 to 0.832). The cut-off corresponding to equal values of sensitivity and specificity, as well as the DOR and GDA estimates, are shown in Figure 6, while the corresponding bias b, obtained according to equation (8), and the expected GDA are reported in Supplementary Material 2. With regard to Cyfra21-1, the corresponding ROC curve (Figure 6) was clearly asymmetrical, with a statistically significant departure from the theoretical proper model (p=0.003, Metz and Kronman test). Thus, to compare the 2 ROC curves, a test for the comparison between 2 pAUCs could be more appropriate than a standard test for the corresponding whole AUCs. For instance, in the specificity range of 0.80 to 1.00, the difference between the 2 corresponding pAUCs was 0.070 and the corresponding p-value was highly statistically significant (p<0.001). Applying a standard test for the comparison of the AUCs, the difference between the 2 corresponding whole AUCs was only marginally statistically significant (p=0.043) (Figure 6).
- Comparison between 2 proper receiver operating characteristic curves
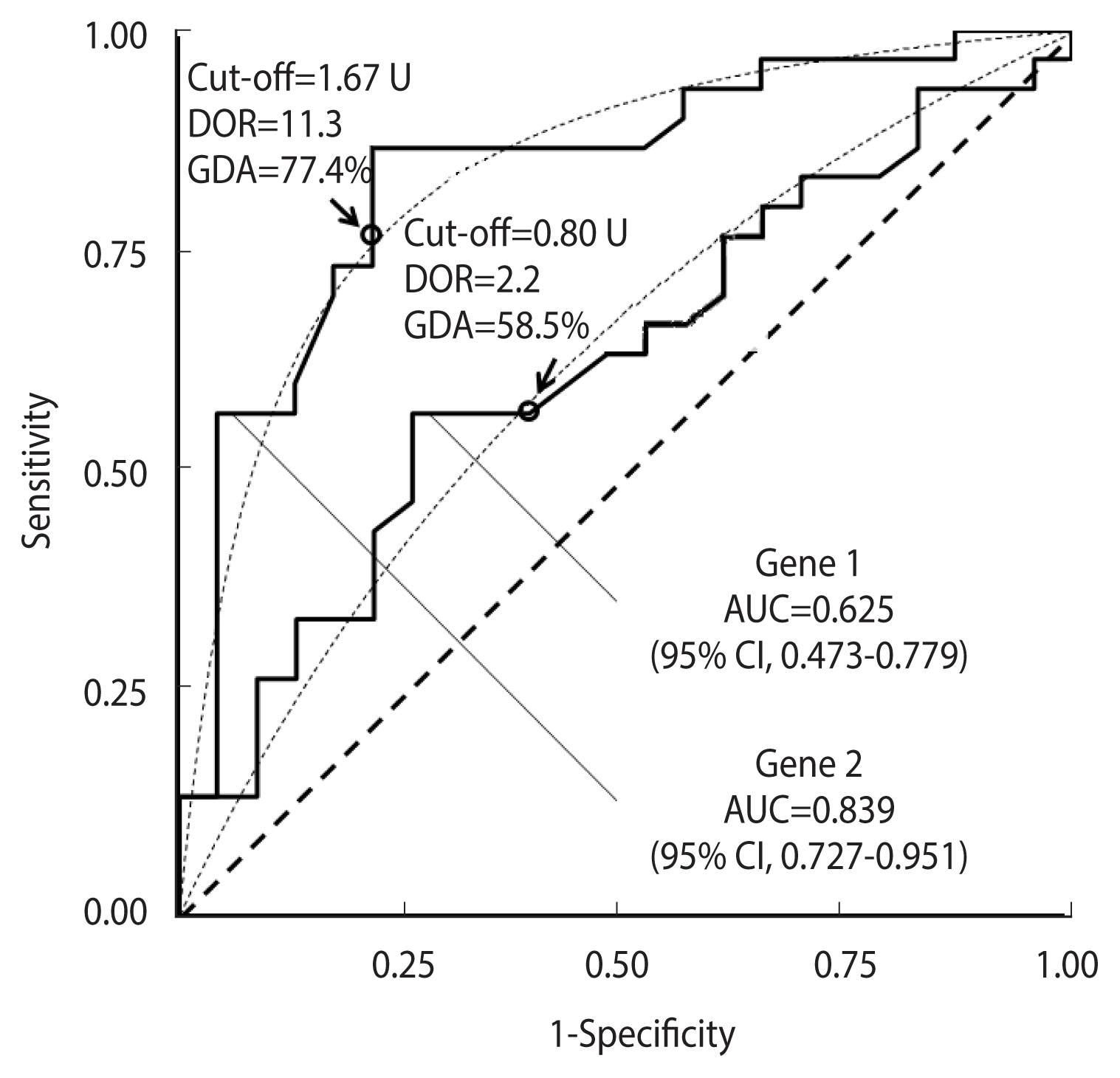
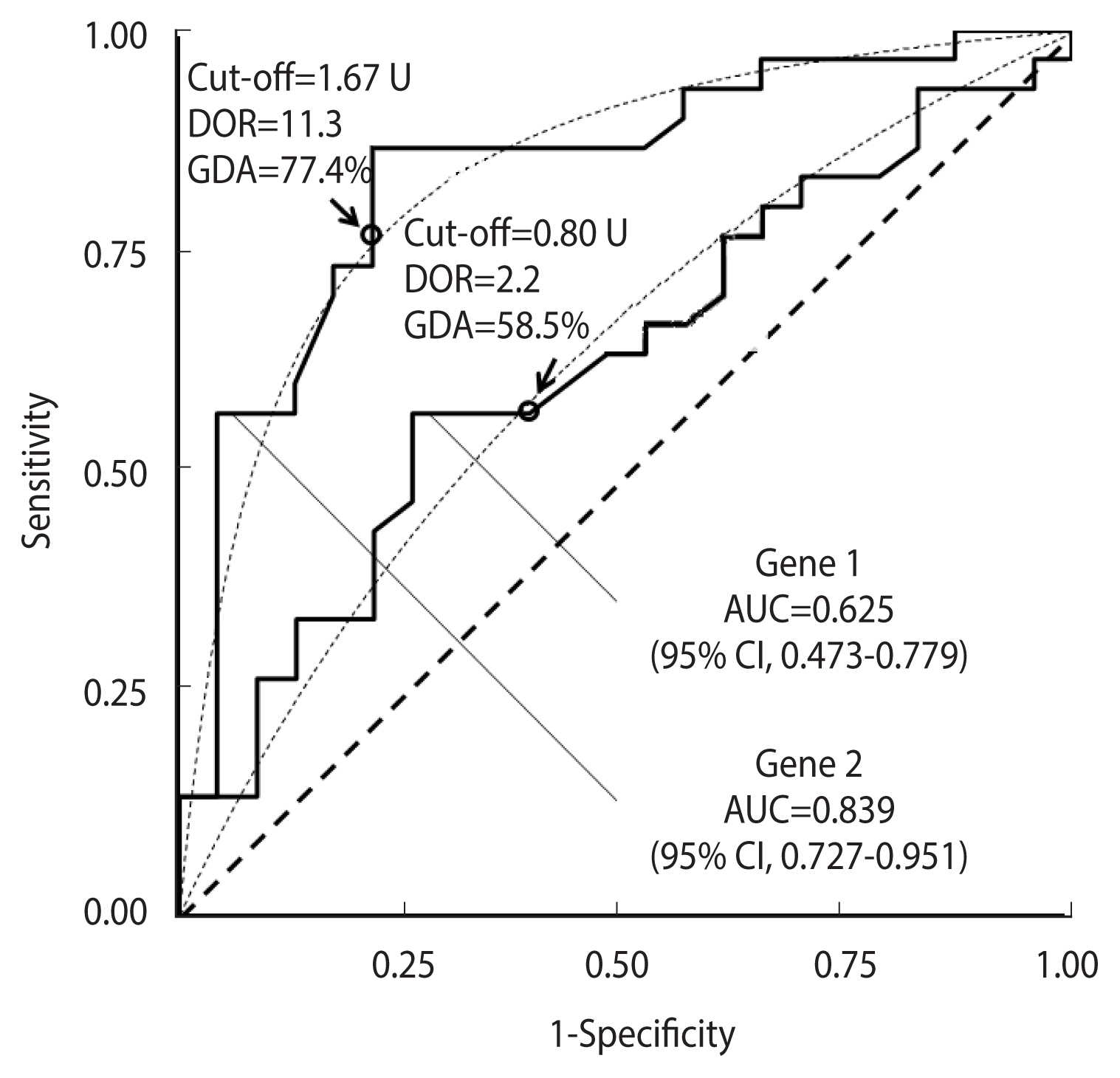
- Figure 7 shows a comparison between the ROC curves corresponding to the expression of the first 2 genes in the “ovarian cancer” dataset.
- The AUC for gene 1 was 0.625 (95% CI, 0.473 to 0.779), and that for gene 2 was 0.839 (95% CI, 0.727 to 0.951). The cut-offs corresponding to equal values of sensitivity and specificity, and the DOR and GDA estimates are also displayed. The corresponding bias b, estimated according to equation (8), and the expected GDA are reported in Supplementary Material 2.
- Both empirical curves fitted the theoretical plot quite well (p=0.546 for gene 1 and p=0.645 for gene 2, respectively), indicating that the comparison of the 2 whole AUCs was appropriate. The test result (p=0.027) suggested that the performance of gene 2 could be higher than that of gene 1 when used as a DM for the diagnosis of ovarian cancer. Conversely, if a test for the 2 corresponding pAUCs in the specificity range of 0.80–1.00 had been applied, a p-value of 0.141 would have been obtained (Figure 7).
RESULTS
- Since its first application in clinical epidemiology in the early 1980s [25], ROC analysis has become an increasingly popular method to assess the performance of DMs, which in combination with patients’ clinical and demographic characteristics provides valid support for the differential diagnosis of several diseases [5]. However, the use of the AUC for diagnostic applications has often been criticised for many reasons, including the fact that the connection between the AUC and the probability of a correct classification remains unclear [4,5]. We have demonstrated that the AUC represents an upper limit of the expected global accuracy at an optimal cut-off and for balanced groups. In proper curves, the actual GDA at an optimal cut-off can be obtained from the AUC, and it is independent from the proportion of cases in the studied sample. The latter property may have important clinical consequences, because the accuracy of a DM at an optimal cut-off can be estimated using a suitable sampling ratio, provided that cases and controls are representative of the general population of diseased and non-diseased individuals, respectively. However, the choice of a suitable cut-off depends on the costs associated with false-positive and false-negative results and the expected proportion of diseased subjects in the target population [26]. In this case, the clinical usefulness of AUC remains to be clarified.
- An interesting property of proper ROC curves is that the comparison between 2 pAUCs can be performed by a test for 2 AUCs with a strong improvement of the statistical power. We applied the Metz and Kronman test [18] to distinguish between proper and non-proper ROC curves, which could guide the choice of the most suitable approach for the comparison of 2 curves.
- The results of the present investigation strongly support the statement by Janssens & Martens [5] that AUC should always be interpreted considering the shape of the entire ROC curve, which mirrors the performance of the underlying marker at different ranges of values. A proper model implicitly assumes that the disease is associated with an increase in DM values that is homogeneous within the group of cases [8]. In the presence of strong departures from the proper model, the AUC no longer provides a useful measure of the potential performance of the underlining diagnostic marker, and some new ROC-based parameters have recently been proposed, including the area under a generalised ROC curve [27] and the length of a ROC curve [28]. Moreover, a departure from the assumption of a proper curve may reflect the presence of heterogeneous subgroups among either group under study. For example, wiggly ROC curves may indicate the presence of hidden subgroups inside either analysed group [8,29–31], while asymmetric curves that do not cross the line of chance may indicate that only a subgroup of cases differs from controls for the presence of higher DM values [32,33]. Finally, the loss of concavity in empirical curves can be quite common even if the corresponding theoretical ROC curve is concave [16]. In such a case, the corresponding AUC estimate can be affected by a negligible bias, whereas the pAUC is more likely to be overestimated or underestimated [16]. Further investigations are needed to develop new methods to identify concave non-symmetric ROC curves, and to elucidate the relationship between the AUC and GDA.
- The results of this study should be considered in light of some limitations. ROC analysis has been criticised when applied to analyse risk score profiles in that a clinically significant change in the probability of disease for 1 or more subjects (the risk estimate) might not be reflected by an appreciable increase in the corresponding AUC [5,34]. Furthermore, the usefulness of ROC analysis for assessing the improvement in prediction performance gained by adding a DM to a baseline predictor remains controversial, even though some alternatives recently proposed have been criticised as well [35].
- In conclusion, our study indicates that the AUC is a useful measure of accuracy with potential clinical relevance for the evaluation of DMs and that it represents an upper limit of disease accuracy when the curve shape is consistent with the binomial proper model. In this case, the GDA at an optimal cut-off is independent from the sampling ratio, thus favouring the design of suitable studies for the evaluation of potential diagnostic markers. Finally, for binormal proper curves, a statistical comparison between 2 or more pAUCs is equivalent to the comparison of the corresponding whole AUCs, which has a higher statistical power. ROC parameters, including the AUC and the pAUC, should always be evaluated in combination with an analysis of the shape of the corresponding ROC curve.
DISCUSSION
SUPPLEMENTARY MATERIALS
ACKNOWLEDGEMENTS
-
DATA AVAILABILITY
The “GH deficit” dataset includes marker values that are reported in a related paper (Secco et al., 2009). Data in the “malignant mesothelioma” dataset are not publicly available, but the corresponding ROC curves used to illustrate our method have been reported in Figure 2 of the article by Filiberti et al. (2013) [24]. Finally, gene expression in the “ovarian cancer” dataset is publicly available on the website of the Fred Hutchinson Cancer Research Center at the website: https://research.fredhutch.org/diagnostic-biomarkers-center/en/datasets.html.
-
CONFLICT OF INTEREST
The authors have no conflicts of interest to declare for this study.
-
FUNDING
None.
-
AUTHOR CONTRIBUTIONS
Conceptualization: Parodi S. Data curation: Parodi S. Formal analysis: Parodi S, Verda D. Funding acquisition: None. Methodology: Parodi S. Project administration: Muselli M. Visualization: Parodi S, Verda D, Bagnasco F, Muselli M. Writing – original draft: Parodi S. Writing – review & editing: Parodi S, Verda D, Bagnasco F, Muselli M.
NOTES

- 1. Bamber D. The area above the ordinal dominance graph and the area below the receiver operating characteristic graph. J Math Psychol 1975;12:387-415.Article
- 2. Janes H, Longton G, Pepe M. Accommodating covariates in ROC analysis. Stata J 2009;9:17-39.PubMedPMC
- 3. Pepe M, Longton G, Janes H. Estimation and comparison of receiver operating characteristic curves. Stata J 2009;9:1.ArticlePubMedPMCPDF
- 4. Vickers AJ. Incorporating clinical considerations into statistical analyses of markers: a quiet revolution in how we think about data. Clin Chem 2016;62:671-672.ArticlePubMedPDF
- 5. Janssens AC, Martens FK. Reflection on modern methods: revisiting the area under the ROC curve. Int J Epidemiol 2020;49:1397-1403.ArticlePubMedPDF
- 6. McClish DK. Analyzing a portion of the ROC curve. Med Decis Making 1989;9:190-195.ArticlePubMedPDF
- 7. Jiang Y, Metz CE, Nishikawa RM. A receiver operating characteristic partial area index for highly sensitive diagnostic tests. Radiology 1996;201:745-750.ArticlePubMed
- 8. Pepe MS. The statistical evaluation of medical tests for classification and prediction. Oxford: Oxford University Press; 2003. p 65-129.
- 9. Robin X, Turck N, Hainard A, Tiberti N, Lisacek F, Sanchez JC, et al. pROC: an open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinformatics 2011;12:77.ArticlePubMedPMCPDF
- 10. Bandos AI, Guo B, Gur D. Jackknife variance of the partial area under the empirical receiver operating characteristic curve. Stat Methods Med Res 2017;26:528-541.ArticlePubMedPMCPDF
- 11. Ma H, Bandos AI, Gur D. On the use of partial area under the ROC curve for comparison of two diagnostic tests. Biom J 2015;57:304-320.ArticlePubMed
- 12. R Core Team. An introduction to R version 4.1.2. [cited 2022 Oct 31]. Available from: https://www.R-project.org/ .
- 13. Pepe MS, Etzioni R, Feng Z, Potter JD, Thompson ML, Thornquist M, et al. Phases of biomarker development for early detection of cancer. J Natl Cancer Inst 2001;93:1054-1061.ArticlePubMed
- 14. Eusebi P. Diagnostic accuracy measures. Cerebrovasc Dis 2013;36:267-272.ArticlePubMedPDF
- 15. Pepe MS, Janes H, Longton G, Leisenring W, Newcomb P. Limitations of the odds ratio in gauging the performance of a diagnostic, prognostic, or screening marker. Am J Epidemiol 2004;159:882-890.ArticlePubMed
- 16. Bandos AI, Guo B, Gur D. Estimating the area under ROC curve when the fitted binormal curves demonstrate improper shape. Acad Radiol 2017;24:209-219.ArticlePubMed
- 17. Metz CE, Pan X. “Proper” binormal ROC curves: theory and maximum-likelihood estimation. J Math Psychol 1999;43:1-33.ArticlePubMed
- 18. Metz CE, Kronman HB. Statistical significance tests for binormal ROC curves. J Math Psychol 1980;22:218-243.Article
- 19. Dorfman DD, Berbaum KS, Metz CE, Lenth RV, Hanley JA, Abu Dagga H. Proper receiver operating characteristic analysis: the bigamma model. Acad Radiol 1997;4:138-149.ArticlePubMed
- 20. Walter SD. Properties of the summary receiver operating characteristic (SROC) curve for diagnostic test data. Stat Med 2002;21:1237-1256.ArticlePubMed
- 21. DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics 1988;44:837-845.ArticlePubMed
- 22. Walter SD. The partial area under the summary ROC curve. Stat Med 2005;24:2025-2040.ArticlePubMed
- 23. Secco A, di Iorgi N, Napoli F, Calandra E, Calcagno A, Ghezzi M, et al. Reassessment of the growth hormone status in young adults with childhood-onset growth hormone deficiency: reappraisal of insulin tolerance testing. J Clin Endocrinol Metab 2009;94:4195-4204.ArticlePubMed
- 24. Filiberti R, Parodi S, Libener R, Ivaldi GP, Canessa PA, Ugolini D, et al. Diagnostic value of mesothelin in pleural fluids: comparison with CYFRA 21–1 and CEA. Med Oncol 2013;30:543.ArticlePubMedPDF
- 25. Erdreich LS, Lee ET. Use of relative operating characteristic analysis in epidemiology. a method for dealing with subjective judgement. Am J Epidemiol 1981;114:649-662.PubMed
- 26. Baker SG, Kramer BS. Peirce, Youden, and receiver operating characteristic curves. Am Stat 2007;61:343-346.Article
- 27. Martínez-Camblor P, Pérez-Fernández S, Díaz-Coto S. The area under the generalized receiver-operating characteristic curve. Int J Biostat 2021;18:293-306.ArticlePubMed
- 28. Bantis LE, Tsimikas JV, Chambers GR, Capello M, Hanash S, Feng Z. The length of the receiver operating characteristic curve and the two cutoff Youden index within a robust framework for discovery, evaluation, and cutoff estimation in biomarker studies involving improper receiver operating characteristic curves. Stat Med 2021;40:1767-1789.ArticlePubMedPMCPDF
- 29. Kagaris D, Yiannoutsos CT. A multi-index ROC-based methodology for high throughput experiments in gene discovery. Int J Data Min Bioinform 2013;8:42-65.ArticlePubMed
- 30. Lee WC, Hsiao CK. Alternative summary indices for the receiver operating characteristic curve. Epidemiology 1996;7:605-611.ArticlePubMed
- 31. Parodi S, Pistoia V, Muselli M. Not proper ROC curves as new tool for the analysis of differentially expressed genes in microarray experiments. BMC Bioinformatics 2008;9:410.ArticlePubMedPMCPDF
- 32. Pepe MS, Longton G, Anderson GL, Schummer M. Selecting differentially expressed genes from microarray experiments. Biometrics 2003;59:133-142.ArticlePubMed
- 33. Parodi S, Muselli M, Carlini B, Fontana V, Haupt R, Pistoia V, et al. Restricted ROC curves are useful tools to evaluate the performance of tumour markers. Stat Methods Med Res 2016;25:294-314.ArticlePubMedPDF
- 34. Cook NR. Use and misuse of the receiver operating characteristic curve in risk prediction. Circulation 2007;115:928-935.ArticlePubMed
- 35. Pepe MS, Fan J, Feng Z, Gerds T, Hilden J. The net reclassification index (NRI): a misleading measure of prediction improvement even with independent test data sets. Stat Biosci 2015;7:282-295.ArticlePubMedPMCPDF
REFERENCES
Appendix
Appendix 1
Figure & Data
References
Citations
- Interpretable machine learning for predicting chronic kidney disease progression risk
Jin-Xin Zheng, Xin Li, Jiang Zhu, Shi-Yang Guan, Shun-Xian Zhang, Wei-Ming Wang
DIGITAL HEALTH.2024;[Epub] CrossRef - Identification of key signaling pathways and hub genes related to immune infiltration in Kawasaki disease with resistance to intravenous immunoglobulin based on weighted gene co-expression network analysis
Yue Wang, Yinyin Cao, Yang Li, Meifen Yuan, Jin Xu, Jian Li
Frontiers in Molecular Biosciences.2023;[Epub] CrossRef -
Escherichia coli
triggers α-synuclein pathology in the
LRRK2
transgenic mouse model of PD
Dongxiao Liang, Han Liu, Ruoqi Jin, Renyi Feng, Jiuqi Wang, Chi Qin, Rui Zhang, Yongkang Chen, Jingwen Zhang, Junfang Teng, Beisha Tang, Xuebing Ding, Xuejing Wang
Gut Microbes.2023;[Epub] CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite