Articles
- Page Path
- HOME > Epidemiol Health > Volume 44; 2022 > Article
-
Systematic Review
Non-cancer health risks in firefighters: a systematic review -
Jeong Ah Kim1
 , Soo Yeon Song1, Wonjeong Jeong1, Jae Kwan Jun1,2
, Soo Yeon Song1, Wonjeong Jeong1, Jae Kwan Jun1,2 -
Epidemiol Health 2022;44:e2022109.
DOI: https://doi.org/10.4178/epih.e2022109
Published online: November 16, 2022
1National Cancer Control Institute, National Cancer Center, Goyang, Korea
2Graduate School of Cancer Science and Policy, National Cancer Center, Goyang, Korea
- Correspondence: Jae Kwan Jun National Cancer Control Institute, National Cancer Center, 323 Ilsan-ro, Ilsandong-gu, Goyang 10408, Korea E-mail: jkjun@ncc.re.kr
© 2022, Korean Society of Epidemiology
This is an open-access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
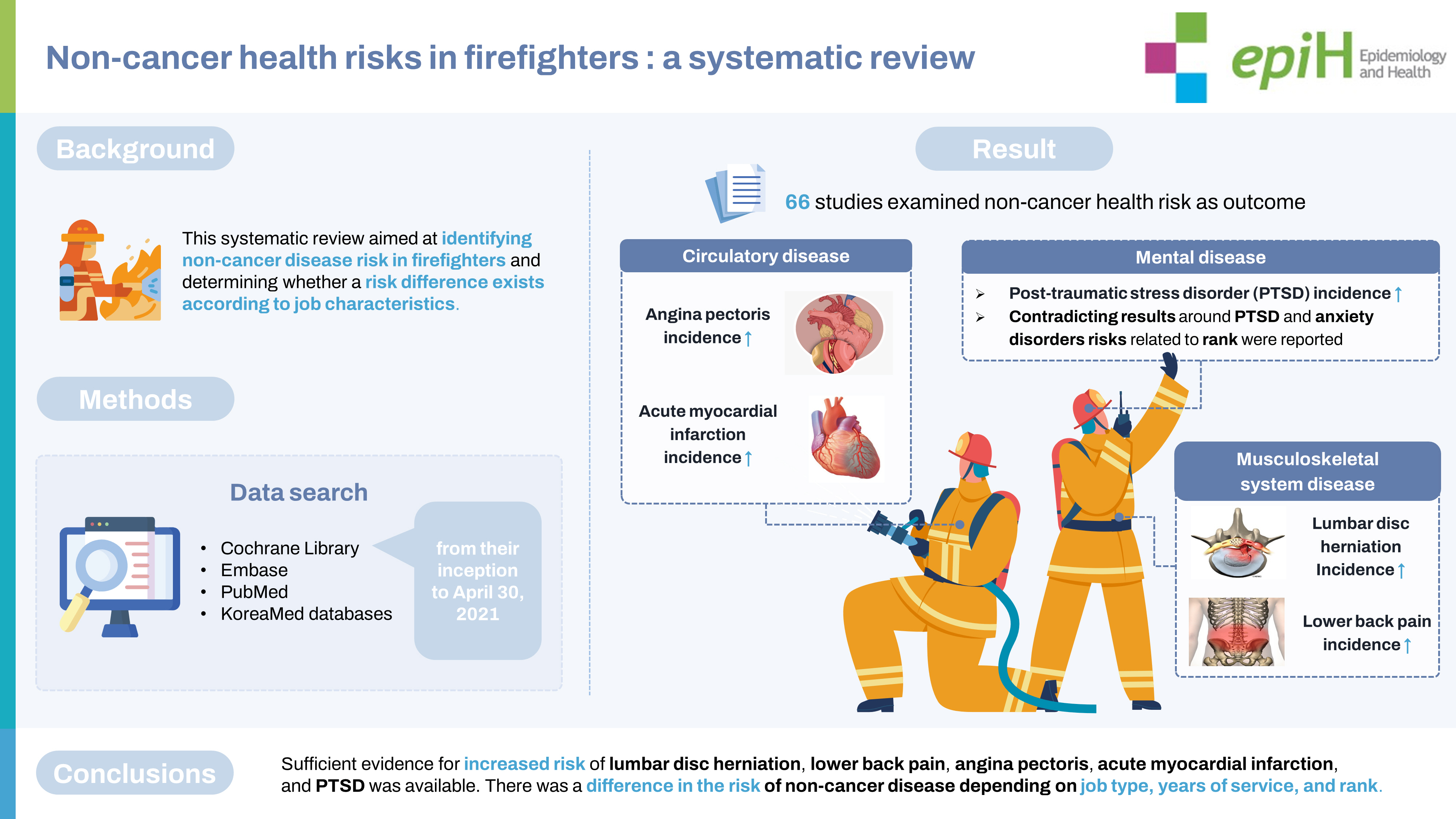
- osFirefighters are occupationally exposed to hazardous factors that may increase their risk of disease. However, non-cancer disease risk in firefighters has not been systematically examined. This systematic review aimed to identify non-cancer disease risk in firefighters and determine whether the risk differs according to job characteristics. We searched the Cochrane Library, Embase, PubMed, and KoreaMed databases using relevant keywords from their inception to April 30, 2021. The Risk of Bias Assessment Tool for Non-randomized Studies version 2.0 was used to assess the quality of evidence. Due to study heterogeneity, a narrative synthesis was presented. The systematic literature search yielded 2,491 studies, of which 66 met the selection and quality criteria. We confirmed that the healthy worker effect is strong in firefighters as compared to the general population. We also identified a significant increase in the incidence of lumbar disc herniation, lower back pain, angina pectoris, acute myocardial infarction, and post-traumatic stress disorder (PTSD) in firefighters compared to other occupational groups. Contradictory results for the risk of PTSD and anxiety disorders related to rank were reported. Sufficient evidence for increased risk of lumbar disc herniation, lower back pain, angina pectoris, acute myocardial infarction, and PTSD was available. The risk of non-cancer diseases varied depending on job type, years of service, and rank. However, caution should be exercised when interpreting the results because the classification criteria for firefighters’ jobs and ranks differ by country.
- Firefighters prevent, take precautions against, or suppress fires and safeguard the lives, bodies, and properties of citizens by providing rescue and first-aid services. During fire suppression activities, firefighters are exposed to a variety of hazardous chemicals, such as smoke, particulate matter, and many other organic toxicants. Most of their working hours are on standby for shift work; thus, they are exposed to job stress. As a result, firefighters face an increased risk of respiratory, cardiovascular, mental, and cancerous disease [1,2]. Determining diseases with a higher risk of incidence and mortality in firefighters is important for prevention, intervention, and occupational safety.
- Most epidemiological studies have examined cancer in firefighters compared with the general population [3-9]. Unfortunately, firefighters have a relatively high cancer incidence and mortality [10-12]. LeMasters et al. [11] reported that firefighters have a probable higher risk of multiple myeloma, non-Hodgkin lymphoma, prostate cancer, and testicular cancer. Similarly, the International Agency for Research on Cancer identified statistically significant increased risks of prostate cancer, testicular cancer, and non-Hodgkin lymphoma in firefighters [12].
- However, relatively few studies have systematically reviewed non-cancer diseases. Although a systematic review of non-cancer diseases in firefighters has been previously published [13], it covered only some non-cancer diseases, such as cardiovascular disease, hearing loss (HL), mental health, respiratory illness, hip osteoarthritis, and sarcoidosis. Therefore, a more comprehensive examination of non-cancer diseases is needed. This study expanded the scope of non-cancer diseases and included studies dealing with symptoms such as pain expressed by firefighters. Hence, we systematically reviewed the literature on the incidence of non-cancer diseases in firefighters as compared to non-firefighters. Furthermore, we investigated whether the risk of noncancer diseases differs depending on job characteristics, such as job type, years of service, and rank.
INTRODUCTION
- Study selection
- This systematic review aimed to identify the risk of non-cancer diseases in firefighters. This study was conducted according to the guidelines of the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) [14,15]. The inclusion criteria for participants, intervention, comparison, outcomes, and study design (PICO-SD) conformed to the specifications suggested by PRISMA [14]. The participants (P) included both male and female firefighters; the intervention (I) included firefighter work; the comparison (C) included (1) inter-comparisons (comparisons of firefighters with non-firefighters) and (2) intra-comparisons (comparisons of firefighters according to job characteristics); the outcomes (O) included non-cancer diseases; and the study design (SD) included cross-sectional, case-control, and cohort studies. Articles were excluded if they met any of the following criteria: (1) were in languages other than English or Korean; (2) evaluated simulation fire experiments or 911 terrorist incidents; (3) did not include comparisons; and (4) were not available as full-text articles.
- Search strategy
- This review was performed in accordance with the PRISMA statement [14]. We searched the Cochrane Library, Embase, PubMed, and KoreaMed databases from database inception up to April 30, 2021, to identify the risk of non-cancer diseases in firefighters. Our search terms included firefighter, disease, incidence, prevalence, mortality, injury, death, and occupational level. Supplementary Material 1 presents the database search strategies.
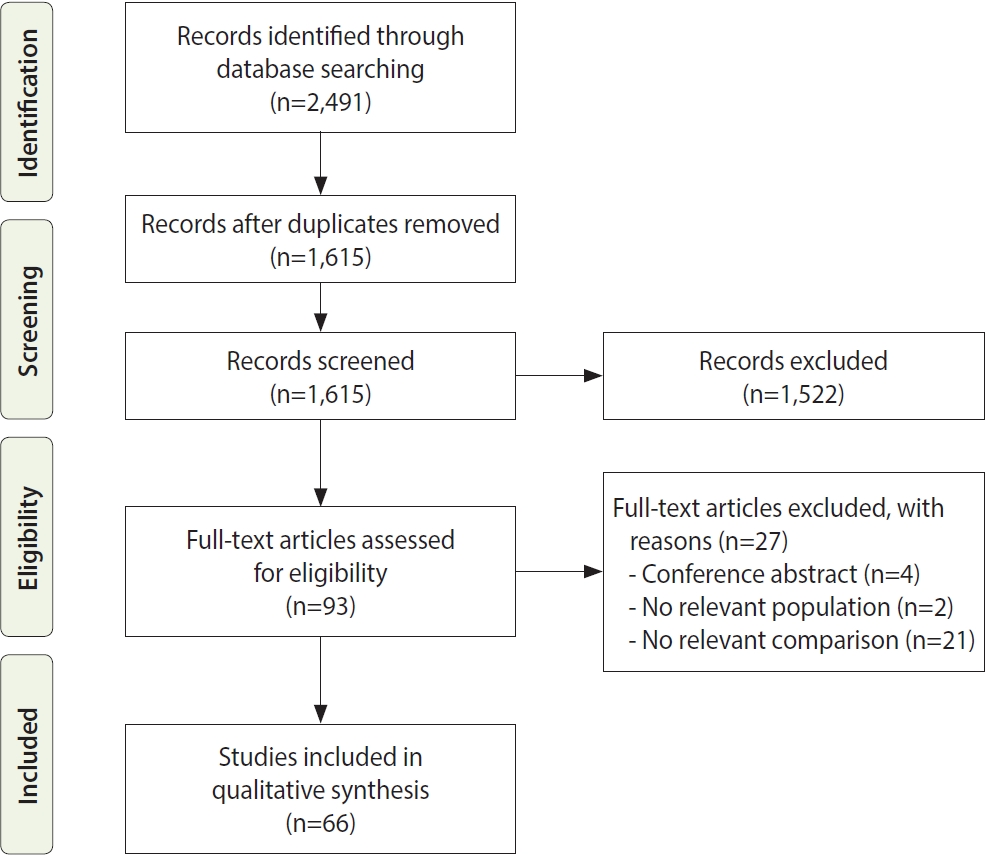
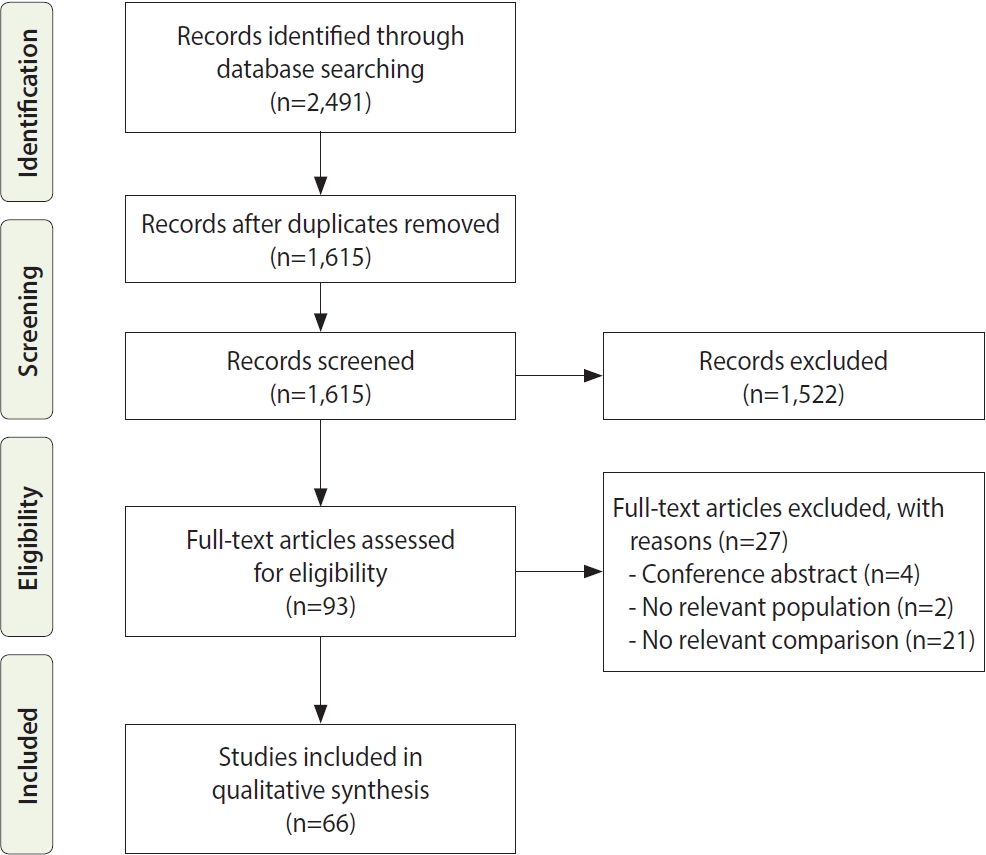
- We identified 2,491 records in the database search and excluded 876 duplicate results. The authors screened the remaining 1,615 records for eligibility and identified 93 articles eligible for full-text review. We excluded 27 studies from the full-text review because they included no comparative group, did not evaluate firefighters as a population, or were only conference abstracts. After a full-text review, 66 studies were included because they met the inclusion and exclusion criteria [16-81].
- The study selection process and results at each stage are summarized in the modified PRISMA flow diagram in Figure 1 [14]. To ensure the validity and reliability of the results, two investigators independently screened the titles and abstracts of the articles and assessed the full texts for eligibility. Discrepancies were resolved through a consensus meeting with a third investigator.
- Quality assessment
- Methodological quality was assessed using the Risk of Bias Assessment Tool for Non-randomized Studies (RoBANS version 2.0) [15]. RoBANS version 2.0 addresses 8 domains: (1) the possibility of target group comparisons, (2) target group selection, (3) confounders, (4) exposure measurement, (5) assessors’ bias, (6) outcome assessment, (7) incomplete outcome data, and (8) selective outcome reporting [15]. Each domain was evaluated as “low risk of bias,” “high risk of bias,” or “unclear.” Two review authors independently applied the tool to each included study and recorded supporting information and justifications for judgment of the risk of bias for each domain. Any discrepancies in judgments of risk of bias or justifications for judgments were resolved by discussion to reach a consensus between the 2 review authors, with a third review author acting as an arbiter if necessary. The results of the quality assessment were presented using Review Manager 5.4 (RevMan; Cochrane Collaboration, Oxford, UK).
- Data extraction and synthesis
- One review author independently extracted all data from the eligible studies, and the characteristics of the variables were systematically organized using a coding table. The coding table included study information (author and publication year), participants (total number of participants, age, and sex), comparison group, study design, diagnostic criteria, and outcomes. This study coded studies as including male or female or both male and female firefighters in relation to sex, and no study recruited only female firefighters. The diagnostic criteria are presented in Supplementary Material 2. Our study used different measures of effect size, such as the standardized mortality ratio (SMR), standardized incidence ratio (SIR), relative risk (RR), hazard ratio (HR), odds ratio (OR), prevalence ratio (PR), incidence density ratio (IDR), and the proportionate mortality ratio (PMR), along with their 95% confidence intervals (CIs). We used the criteria for SMR, IDR, or PMR as follows: If a study reported results by multiplying the SMR, IDR, or PMR by 100, the corresponding result was divided by 100.
- Due to the heterogeneity of diagnostic criteria, comparison groups, and outcomes, the findings are presented as a narrative synthesis. We created outcome categories, and overall non-cancer disease incidence and non-cancer disease mortality rates were analyzed separately. We then organized the studies according to the comparison groups. This process provided a basis for determining the studies that were eligible for each outcome.
- Ethic statement
- This study was approved by the Institutional Review Board of the National Cancer Center in Korea (IRB No. NCC2021-0262).
MATERIALS AND METHODS
- Quality of included reviews
- We used the RoBANS version 2.0 to assess the risk of bias for each of the included studies. Supplementary Material 3 provides a summary of these assessments. Overall, the risk of bias was rated as low or unclear in most identified reviews. Seventeen studies (26%) had a high risk of bias due to an improper selection of target group comparisons, 2 studies (3%) had a high risk of bias due to improper target group selection, 5 studies (8%) had a high risk of bias due to improper consideration related to confounders, 18 studies (27%) had a high risk of bias due to improper exposure measurement, 8 studies (12%) had a high risk of bias due to improper outcome assessment, and 7 studies (11%) had a high risk of bias due to improper handling of incomplete outcome data. Furthermore, in incomplete outcome data and selective outcome reporting, more studies were rated as “unclear” or “high” than as “low.”
- General characteristics of the selected studies
- The general characteristics of the eligible studies are summarized in Table 1 in order of publication year. The largest number of published papers originated from the United States (n= 26), followed by Korea (n= 17), and Denmark (n= 5). The average number of firefighters included in each study was 6,103, and there was a significant difference between studies, from a minimum of 86 to a maximum of 45,698. Most studies involved male firefighters (n = 36). Twenty-seven studies involved both male and female. The age groups varied, with most being within the 20-year-old to 60-year-old range. In terms of inter-comparisons, firefighters were compared to the general population, general employees, police officers, military officers, national and regional government officers (NRGs), hospital office workers (HOWs), office workers, and operating engineers. Intra-comparisons examined job type, service years, and rank.
- Twelve categories of non-cancer diseases in firefighters
- Given the complexity of the outcome, we categorized non-cancer diseases into 12 categories: (1) infectious and parasitic diseases, (2) endocrine diseases, (3) mental diseases, (4) nervous system diseases, (5) hearing impairment and deafness, (6) circulatory diseases, (7) respiratory diseases, (8) gastrointestinal diseases, (9) musculoskeletal system diseases, (10) genitourinary diseases, (11) suicidal behavior, and (12) other diseases.
- We addressed two main outcomes: incidence and mortality. The main outcomes of the eligible studies are summarized in Table 2. Table 2 has also been structured by outcome categories, within which studies are ordered by publication year.
- Infectious and parasitic diseases
- Ten studies identified specific infectious and parasitic diseases [16-25]. In inter-comparisons, most studies indicated a risk decrease ranging from 0.16 to 0.42 in terms of infectious diseases in male firefighters compared to the general population [16,21,23,24]. Male firefighters had significantly lower tuberculosis mortality rates than the general population [17], but 1 study did not show significant results [21]. Moreover, firefighters had a higher seroprevalence of hepatitis C antibodies detected in immunoassays than police officers [20].
- Endocrine diseases
- Twelve studies regarding endocrine diseases were identified [16,17,19,21,23-30]. Concerning inter-comparisons, most studies indicated a significant decrease (0.10 to 0.67) in the endocrine disease SMR in male firefighters compared to the general population, employees, and military [21,23-25]. Furthermore, most studies reported that the mortality rates of diabetes in male firefighters were lower than those in the general population and employees [16,17,21,23,25,30]. The prevalence of diabetes was lower in male firefighters than in non-firefighters [26]. Furthermore, firefighters had lower risks of diabetes mellitus and type 2 diabetes mellitus than NRGs [29].
- Mental diseases
- Eighteen studies that examined mental diseases were identified [19,21,24,25,29,31-43]. Regarding inter-comparisons, male firefighters had significantly higher mortality rates of mental illnesses than the general population in 1 study [19]; compared with NRGs, firefighters had a higher risk of mental illnesses (HR, 1.11; 95% CI, 1.08 to 1.13), mood disorders (HR, 1.12; 95% CI, 1.08 to 1.16), and post-traumatic stress disorder (PTSD; HR, 1.40; 95% CI, 1.26 to 1.56) [29]. The age-standardized prevalence of mental disorders in firefighters was slightly, but not significantly higher, than in government officials and police officers [38]. Deceased firefighters were less likely to have been diagnosed with depression but more likely to have been diagnosed with PTSD than non-firefighters [41].
- Concerning job types, emergency medical service (EMS) personnel had a higher rate of PTSD than administration department personnel (OR, 3.68; 95% CI, 1.47 to 9.23) [32]. The risk of PTSD was the highest among paramedics and rescue workers [39]. Retired firefighters reported significantly higher rates of probable PTSD (OR, 2.61; 95% CI, 1.47 to 4.64) and depression (OR, 4.31; 95% CI, 2.27 to 8.22) than current firefighters [35]. Moreover, the risks of severe depression and anxiety disorder were highest among retired firefighters [39]. Professional firefighters have higher excessive daytime sleepiness (EDS) than volunteer firefighters [43]. However, professional firefighters who worked only as firefighters had a significantly lower probability of suffering from PTSD than firefighters who worked temporarily (OR, 0.30; 95% CI, 0.10 to 0.90) [36].
- Regarding rank, firefighters at a lower rank were more likely to experience complex PTSD (OR, 1.78; 95% CI, 1.01 to 3.13) [42] and had higher rates of depression [40]; this contrasts with the trend observed for anxiety disorders, where the OR for sergeants was 2.20 (95% CI, 1.06 to 4.57) compared to privates [37]. However, another study reported no significant differences in the prevalence of anxiety disorders according to rank [40].
- Nervous system disease
- Thirteen studies have examined nervous system diseases in firefighters [19,21,24,25,29,30,39,43-48]. Regarding inter-comparison, most studies indicated a decrease ranging between 0.47 and 0.68 in nervous system disease risk in male firefighters compared to the general population and employees [21,24,25,44]. Firefighters had a higher risk of sleep disorder (HR, 1.04; 95% CI, 1.01 to 1.08) compared with NRGs [29]. Furthermore, the proportion of firefighters with mild and severe insomnia was higher than HOWs [47].
- Concerning the job types, the OR of insomnia was 2.45 (95% CI, 1.46 to 4.12) for fire suppression and 1.87 (95% CI, 1.10 to 3.16) for EMS and rescue personnel [48]. Among the types of duties, the risk of poor sleep quality was the highest among office administrators [39]. Regarding years of service, the ratio of poor sleep significantly decreased with the length of service. It was highest at 52.5% in firefighters with less than 10 years of service, followed by 51.3% in those with 10 years to 20 years of service, and lowest at 37.7% in firefighters with more than 20 years of service [45].
- Hearing impairment and deafness
- Seven studies examined hearing impairments and deafness [34,49-54]. Concerning inter-comparison, male firefighters had HL compared with the age-matched otologically normal population [49]. Moreover, male firefighters’ age-adjusted hearing threshold levels were significantly worse than the otologically normal male population (PR, 5.29; 95% CI, 3.34 to 8.39) [53]. Rescuers also had significantly worse hearing than the non-industrial noise-exposed male Korean population [53]. Regarding intra-comparison, the hearing threshold at 4,000 Hz significantly increased with more years spent on the job [51]. Low and high frequency HL prevalence was significantly higher among firefighters with longer work experience than those with shorter work experience [52].
- Circulatory disease
- Twenty-two studies that explored circulatory disease [16,17,19,21,23-26,29,30,34,38,44,46,55-62]. Concerning inter-comparison, most studies indicated a 0.27 to 0.86 decrease in circulatory disease in male firefighters compared to the general population [16,21,23,24,55]; however, female firefighters had a significantly higher SMR from circulatory disease [21].
- Mortality due to heart disease is significantly lower in male firefighters than in the general population [17], but some studies have reported a lack of association [19,57]. Male firefighters have significantly lower mortality rates from cardiovascular diseases (CVD) than the general population, while female firefighters have significantly higher mortality rates [21]. Most studies reported that the mortality rates of cerebrovascular disease in firefighters was significantly lower than the general population and police officers [19,23,30,44,57,61]. However, firefighters had a significantly higher risk of death or hospitalization from myocardial infarction (MI; HR, 1.24; 95% CI, 1.07 to 1.43) and ischemic stroke (HR, 1.43; 95% CI, 1.12 to 1.82) than the general population [62].
- Compared with male employees, firefighters had a higher risk of angina pectoris (SIR, 1.16; 95% CI, 1.08 to 1.24), acute MI (SIR, 1.16; 95% CI, 1.06 to 1.26), chronic ischemic heart disease (IHD; SIR, 1.15; 95% CI, 1.06 to 1.24) and atrial fibrillation/flutter (SIR, 1.25; 95% CI, 1.14 to 1.36) [46]. Concerning the job types, the OR of mortality from coronary heart disease were 12.1 times to 136.0 times higher in fire suppression personnel, 2.8 times to 14.1 times higher in alarm response personnel, and 2.2 times to 10.5 times higher in alarm return personnel as compared with individuals on non-emergency duties [59]. Furthermore, the risk of sudden cardiac death was significantly increased in firefighters responsible for fire suppression, alarm response, and alarm return [60]. Compared to those with less than 10 years of experience as a wildland firefighter, those with 10-19 years of experience had greater odds of having ever been diagnosed with hypertension (OR, 4.2; 95% CI, 1.3 to 14.0), as did those with 20 or more years of experience (OR, 5.0; 95% CI, 1.3 to 20.2) [34].
- Respiratory disease
- Sixteen studies examining respiratory disease were reviewed [16,17,19,21,23-25,30,34,44,55,57,58,63-65]. Concerning intercomparison, male firefighters had lower mortality rates from respiratory diseases than the general population [16,17,21,23,24,30,44]. The SMR for pneumonia in male firefighters was significantly lower than that in the general population and employees [21,25]; however, unlike male firefighters, female firefighters had a higher but non-significant SMR for pneumonia than the general population [21].
- The SMR for bronchitis, emphysema, and asthma in male firefighters was significantly lower than that of the working population [25]; emphysema deaths in male firefighters were significantly lower than those in the general population [17]. Full-time firefighters had significantly increased asthma rates compared with military personnel (SIR, 1.58; 95% CI, 1.32 to 1.88), while the risk of chronic obstructive pulmonary disease showed no significant results [65].
- Gastrointestinal disease
- Eleven studies discussing gastrointestinal disease have been identified [16,17,19,21,23-25,29,30,44,66]. The SMR for liver disease in male firefighters was significantly lower than that in the general population [23]. Furthermore, the SMR for liver and bile duct diseases in male firefighters was significantly lower than that in non-firefighter male employees [25]. However, compared with the general population, significant increases in cirrhosis and chronic liver disease mortality in firefighters have been consistently reported [17,30].
- Musculoskeletal system disease
- Thirteen studies about musculoskeletal system disease were reviewed [24,29,34,38,47,67-74]. Concerning inter-comparison, male firefighters had significantly lower SMR for musculoskeletal system diseases than the general population [24]. Male firefighters were reported to have a greater likelihood of experiencing facet joint degeneration (FJD) than HOWs at all lumbar spinal levels except for lumbar (L)3-L4 [71]. Furthermore, the proportions of firefighters with herniated disc(s) (L4-L5) and spinal stenosis (L5- S1) were significantly higher than that of HOWs [47]. The OR of lower back pain (LBP) in EMS and rescue personnel was also statistically higher than that in HOWs [47].
- Regarding job types, volunteer firefighters had a 1.7-fold increase in burn-related mortality rate and a 1.8-fold increase in trauma-related mortality than career firefighters [74]. L4-L5 intervertebral disc herniation OR in firefighting, emergency, or rescue personnel was 3.49 (95% CI, 1.24 to 9.86) [70]. EMS and fire suppression workers experienced injuries on duty more often than office workers, and their odds of injuries were three and two times higher, respectively [69].
- Regarding years of service, firefighters with more than 17 years of fire services were more likely to report injuries [67]. Furthermore, during the 13-year follow-up period, the prevalence of radiating and local LBP increased [68]. The prevalence of LBP also increases with the duration of years spent in EMS and emergency rescue work [72].
- Genitourinary disease
- Seven studies examining genitourinary disease were identified and reviewed [16,19,21,24,25,44,75]. Regarding the inter-comparison, most studies indicated a genitourinary disease SMR decrease between 0.38 and 0.54 in male firefighters as compared to the general population [16,21,44]. The SMR for chronic nephritis in male firefighters is lower than that in the general population [16]. The models assessing male-factor infertility yielded the highest HR among full-time firefighters (HR, 1.46; 95% CI, 1.10 to 1.94) in the male. In Vitro Fertilization model and the male National Patient Register model (HR, 1.53; 95% CI, 1.18 to 1.98), compared to employees [75].
- Suicidal behavior
- Twelve studies examined suicidal behavior [16,19,21,23,25,41,44,58,76-79]. Concerning the inter-comparison, firefighters had a higher PMR of 1.72 (95% CI, 1.53 to 1.93) than employees [79]. However, most studies reported that male firefighters have a lower SMR from suicide than the general population [16,19,21,25, 44,58,77], employees, and the military [25]. Mortality due to intentional self-harm was significantly lower among firefighters than among the general population [23]. Intentional self-harm was significantly higher in firefighters employed for over 20 years compared with never-firefighters and firefighters employed for less than 10 years [23]. In contrast, individuals with fewer years of service as firefighters were more likely to report career suicidal ideation, plans, attempts, and non-suicidal self-injury [76]. Furthermore, firefighter decedents had a lower proportion of history of suicide attempts or thoughts than non-firefighter decedents [41].
RESULTS
- We conducted a systematic review to identify the risk of noncancer disease in firefighters. A total of 66 studies were identified in our systematic search of the four main databases. During the literature selection process, we excluded studies related to the World Trade Center (WTC) disaster that occurred on September 11, 2001 [82]. The WTC disaster released a large quantity and variety of toxicants into the environment, affecting rescue and recovery workers as well as community members. As cancers, lung disease, heart disease, and PTSD have been shown to be markedly increased, we excluded them.
- Most studies have included both male and female firefighters. The risk of death for male and female firefighters was not equal compared with the general population. Male firefighters have significantly lower mortality rates from infectious and parasitic diseases, respiratory disease, pneumonia, gastrointestinal disease, and suicide than the general population; however, unlike male fighters, female firefighters’ mortality rates are not significantly different compared to the general population. Furthermore, the SMR for circulatory disease and CVD in female firefighters was significantly higher than that in general population. However, no study has targeted only female firefighters. Since female firefighters do not account for a large proportion of all firefighters, it is difficult to recruit only female firefighters as subjects in studies, and, as a result, in systematic reviews. Literature about female firefighters and the risk of non-cancerous disease currently lacks evidence. Further studies are needed to understand the risk of non-cancerous diseases in this population.
- First, the main results of our study confirmed that the healthy worker effect (HWE) is strong in firefighters as compared with the general population. Firefighters are selected and trained, and so they are expected to be much healthier than the general public. Hence, firefighters are at a lower risk of morbidity and mortality due to disease than the general population. Since most studies had results affected by the HWE, firefighters consistently displayed a lower risk of non-cancer disease than the general population. Therefore, it is essential to match firefighters with an appropriate comparison group to minimize the influence of HWE on statistical analysis and outcomes.
- Second, we found that specific non-cancer disease may occur more frequently in firefighters than in other occupational groups, such as police officers, NRGs, military workers, HOWs, and employees. Police officers and military personnel have demographic characteristics similar to firefighters, with comparable socioeconomic status, access to medical services, and physical condition [83]. However, male firefighters had more deaths from respiratory diseases [55], higher hepatitis C [20], and burnout prevalence [66] compared with police officers. Furthermore, the SMR for congenital malformations of the circulatory system in male firefighters and the incidence of asthma in firefighters was higher than military personnel [25,65].
- Compared with HOWs, male firefighters have a higher prevalence of insomnia, FJD, spinal stenosis, and disc herniation [47,71]. Furthermore, firefighters responsible for rescue and paramedic services have higher LBP than HOWs [47]. This is estimated to increase the likelihood of musculoskeletal disorders, owing to the necessity for rapid use of force and unnatural posture when transporting patients on stretchers [84]. Compared with general employees, male firefighters have a higher incidence of circulatory diseases, such as angina pectoris, acute MI, chronic IHD, atrial fibrillation, and CVD [46]. Furthermore, full-time male firefighters have a higher risk of infertility than workers as hyperthermia, a major firefighting hazard, may impair male fertility [75,85].
- Different studies comparing suicide mortality between firefighter and employees report inconsistent results. Danish firefighters had significantly lower suicide mortality than workers [25], while the United States firefighters had a significantly higher suicide mortality rate than employees [79]. The reason for the disparity between the results seems to be firefighter education on suicide symptoms and prevention, which differs from country to country. Firefighter suicide is a serious problem; from 2011 to 2020, in Korea 97 firefighters attempted suicide; of those, 49 succeeded; approximately twice as many as their deaths [86]. Although the direct cause of firefighter suicide has not been directly linked to the occupation itself, it is estimated that serious mental and physical pain experienced in the field may increase the risk of suicide.
- Third, we confirmed that there was a difference in the risk of non-cancer disease depending on job type, years of service, and rank. Concerning job type, firefighters working on fire suppression, alarm response, and alarm return had high rates of sudden cardiac deaths [60] and coronary artery disease deaths [59]. Rescue and paramedic firefighters were shown to be at high risk of PTSD [32,79] as firefighters often encounter serious conditions and witness the death of patients during their duties [87]. Field firefighters had high insomnia [48] and disc herniation incidences [70], while officers were at high-risk of sleep disorders [39] and suicidal thoughts [78]. Moreover, firefighter decedents were more likely to have been diagnosed with PTSD than non-firefighter decedents [41].
- Retired firefighters experience more emotional problems, such as depression and anxiety disorders [35,39] and have a higher incidence of PTSD, than non-retired firefighters [35]. People who have experienced retirement are psychologically stressed by the feeling that they no longer fulfill an important role and stress and psychological trauma were accumulated [88]. Seasonal firefighters have a higher incidence of PTSD [36]. This is thought to be due to the increased risk of accidents and mental health issues because of the relative lack of professional training, education on trauma response, and experience that professional firefighter have. In contrast, professional firefighters have a higher prevalence of EDS and sleep disorders [43].
- Regarding years of service, the longer firefighters worked, the larger the incidence of deaths from intentional self-harm [23]. Furthermore, the prevalence of hepatitis B [22], HL [51,52], and injuries [67] was higher among those who worked for a long time. We believe that, with longer years of service, capacity for concentration and safety awareness decrease due to aging, which leads to increased accidents. In contrast, the shorter the years of service, the higher the prevalence of sleep disorders [45]. Furthermore, firefighters with fewer years of service were more likely to report suicide attempts, suicidal thoughts, suicide plans, and non-suicide self-harm [76].
- Inconsistent results were found for PTSD related to firefighter rank. In a Korean study using a cross-sectional study, firefighters showed significant differences in PTSD incidence according to ranks [32]. However, in a British study using a cohort study, there were no significant differences [42]. Furthermore, inconsistent results have been found for rank-related anxiety disorders. A Brazilian study showed significant differences in the occurrence of anxiety disorders between firefighter ranks [37], while a Chinese study showed no significant differences [40]. This could be due to the different study designs, social/cultural variances, or both; further research is needed.
- This is the first systematic review that comprehensively analyzes the risk of various non-cancer disease in firefighters. We used recognized literature search methods to minimize the risk of bias in our methodology. These findings appear to be largely in line with a systematic review of non-cancer occupational health risks in firefighters [13]. Inconclusive findings about increased risk of coronary heart disease and respiratory ill-health in firefighters were reported. They also found that the risk of HL, hip and knee osteoarthritis, mental issues, and sarcoidosis increased in firefighters, with limited evidence. This is consistent with our finding that the evidence of various non-cancer disease is insufficient. Although the risk of specific non-cancer disease in firefighters was increased in this study, the evidence for each disease is commonly cited from only one or two studies. More research for further evidence is required.
- This study had several limitations. First, this study was conducted as a descriptive analysis, not a meta-analysis, because of the large heterogeneity of the included studies with respect to the diagnostic criteria, comparison group, and outcome. Differences in the effect size, outcome, and comparison group made it difficult to compare the results of the included studies. Moreover, some were often limited by selection, performance, confirmation, attrition, and reporting biases; which might be interpreted with caution. Second, we limited the publications to those in the English and Korean languages. However, since the majority of scientific literature is published in English, the authors felt that the publication bias caused by limiting selection to only English or Korean was minor.
- Based on the results of our study, we make the following suggestions. Firstly, it is necessary to establish and operate a systematic surveillance system for firefighters. The United States has been operating the National Firefighter Registry since 2020 to monitor and track firefighters to analyze the correlation between occupational exposure and cancer occurrence [89]. A surveillance system that includes musculoskeletal system disease, circulatory disease, and mental disease should be established. To understand the trend of diseases occurring in firefighters over time, it is necessary to collect and investigate data systematically and continuously. This will contribute to the prevention of diseases and improvement of firefighter health. Second, HWE should be considered when comparing firefighters’ health issues with those of non-firefighters. Firefighters should be compared with appropriate occupational groups rather than with the general population.
DISCUSSION
- We found that the risk of diabetes, CVD, cerebrovascular disease, acute respiratory infection, pneumonia, liver disease, and intentional self-harm in male firefighters was significantly lower than that in the general population. These results indicate that HWE is an important factor for firefighters. Furthermore, the incidence of lumbar disc herniation, LBP, angina pectoris, acute MI, and PTSD was consistently reported to be significantly higher in firefighters than in occupational groups. We also found that the risk of non-cancer disease differed depending on job type, years of service, and rank. However, caution should be exercised when interpreting the results. It was difficult to generalize the results because the classification criteria for firefighters’ jobs and ranks differ by country. It is also not possible to generalize these results to all firefighters because the included studies were conducted on males or both males and females. Further studies are needed to determine the risk of non-cancer disease among female firefighters.
CONCLUSION
SUPPLEMENTARY MATERIALS
Supplementary Material 1.
Supplementary Material 2
Supplementary Material 3
-
CONFLICT OF INTEREST
The authors have no conflicts of interest to declare for this study.
-
FUNDING
This research was funded by the National Fire Agency (grant No. 202100180001) and a Grant-in-Aid for Cancer Research and Control from the National Cancer Center of Korea (#2210771).
-
AUTHOR CONTRIBUTIONS
Conceptualization: Jun JK. Data curation: Kim JA. Formal analysis: Kim JA, Song SY. Funding acquisition: Jun JK. Methodology: Kim JA, Song SY, Jeong W, Jun JK. Project administration: Jun JK. Visualization: Kim JA. Writing – original draft: Kim JA, Jeong W. Writing – review & editing: Kim JA, Song SY, Jeong W, Jun JK.
NOTES
ACKNOWLEDGEMENTS

| RN | Sex | Comparison1 | Outcomes related to mortality (95% CI) | Outcomes related to incidence and prevalence (95% CI) | ||
|---|---|---|---|---|---|---|
| (1) Infectious and parasitic diseases | ||||||
| [16] | M | [1] | SMR 0.42 | |||
| [23] | M | [1] | SMR 0.33 (0.04, 1.20) | |||
| [29] | M, F | [1] | Male FF: SMR 0.16 (0.11, 0.22)* | |||
| Female FF: SMR 0.27 (0.00, 1.52) | ||||||
| [45] | M | [1] | SMR 0.30 (0.14, 0.55)* | |||
| [47] | M | [1] | SMR 0.30 (0.16, 0.50)* | |||
| [65] | M | [2], [3] | [2] SMR 0.76 (0.44, 1.31) | |||
| [3] SMR 1.10 (0.64, 1.90) | ||||||
| Tuberculosis | ||||||
| [20] | M | [1] | RR 0.26 (0.07, 0.68)2* | |||
| [29] | M | [1] | SMR 1.10 (0.35, 2.56) | |||
| Hepatitis B virus infection | ||||||
| [22] | M | [1] | FF 4.5%, [1] 6.8% | |||
| [39] | M, F | Length of service, rank | ≥20 yr 19.6%, 10-20 yr 4.2%, <10 yr 3.3%* | |||
| Rank was not associated with a higher prevalence of hepatitis B infection | ||||||
| Hepatitis C virus infection | ||||||
| [27] | M, F | [4] | FF 2.3%, [4] 0.6% | |||
| (2) Endocrine diseases | ||||||
| [29] | M | [1] | SMR 0.35 (0.22, 0.52)* | |||
| [45] | M | [1] | SMR 0.44 (0.25, 0.72)* | |||
| [47] | M | [1] | SMR 0.67 (0.44, 0.98)* | |||
| [65] | M | [2], [3] | [2] SMR 0.10 (0.01, 0.73)* | |||
| [3] SMR 0.12 (0.02, 0.87)* | ||||||
| Diabetes mellitus | ||||||
| [16] | M | [1] | SMR 0.39 | |||
| [20] | M | [1] | RR 0.36 (0.14, 0.75)2* | |||
| [29] | M | [1] | SMR 0.45 (0.26, 0.73)* | |||
| [37] | M | [2] | FF 6.3%*, [2] 14.1%* | |||
| [45] | M | [1] | SMR 0.45 (0.25, 0.75)* | |||
| [60] | M, F | [5] | HR 0.73 (0.69, 0.77)* | |||
| [65] | M | [2], [3] | [2] SMR 0.58 (0.37, 0.89)* | |||
| [3] SMR 0.80 (0.51, 1.24) | ||||||
| [72] | M, F | [1] | SMR 0.73 (0.64, 0.83)* | |||
| Type 2 diabetes mellitus | ||||||
| [60] | M, F | [5] | HR 0.85 (0.82, 0.88)* | |||
| Endocrine disorders | ||||||
| [23] | M | [1] | SMR 0.46 (0.09, 1.37) | |||
| Metabolic syndrome | ||||||
| [54] | M | [6] | FF 14.4%*, [6] 32.6%* | |||
| Clerical: OR 1.15 (0.69, 1.92) | ||||||
| Managerial: OR 1.52 (0.79, 2.89) | ||||||
| Professionals and related: OR 1.20 (0.75, 1.94) | ||||||
| Service: OR 0.63 (0.27, 1.45) | ||||||
| [57] | M | [FF] | Sales: OR 2.34 (1.29, 4.23)* | |||
| Skilled agricultural, fishing: OR 0.84 (0.40, 1.74) | ||||||
| Craft and related trades: OR 0.97 (0.55, 1.72) | ||||||
| Equipment and assembling: OR 1.27 (0.76, 2.12) | ||||||
| Elementary: OR 1.10 (0.53, 2.28) | ||||||
| (3) Mental diseases | ||||||
| [23] | M | [1] | SMR 4.55 (2.74, 7.11)* | |||
| [29] | M | [1] | SMR 0.41 (0.22, 0.68)* | |||
| [47] | M | [1] | SMR 0.57 (0.38, 0.81) | |||
| [60] | M, F | [5] | HR 1.11 (1.08, 1.13)* | |||
| [65] | M | [2], [3] | [2] SMR 0.37 (0.25, 0.57)* | |||
| [3] SMR 0.47 (0.31, 0.71)* | ||||||
| Depression | ||||||
| [33] | M, F | [Other shift work] | Firefighting: OR 1.17 (0.60, 2.30) | |||
| Ambulance: OR 1.55 (0.76, 3.14) | ||||||
| Rescue: OR 1.01 (0.46, 2.20) | ||||||
| [50] | M, F | [<10 yr] | 10-19 yr: OR 1.7 (0.6, 4.4) | |||
| ≥20 yr: OR 0.8 (0.2, 3.4) | ||||||
| [55] | M, F | [Current FF] | Retired FF: unadjusted OR 4.31 (2.27, 8.22)* | |||
| [76] | M, F | Type of duty | School educator: 1.00%, fire-control: 1.79%, paramedics and rescue: 1.88%, office administrator: 1.62%, retirees: 3.95% | |||
| Mood disorder | ||||||
| [60] | M, F | [5] | HR 1.12 (1.08, 1.16)* | |||
| [75] | M, F | [4], [5] | No significant difference in age-adjusted prevalence between the 3 job categories | |||
| Anxiety disorder | ||||||
| [71] | M | [Privates] | Corporal: OR 1.51 (0.70, 3.28) | |||
| Sergeant: OR 2.20 (1.06, 4.57)* | ||||||
| Sub-lieutenant: OR 0.85 (0.10, 7.09) | ||||||
| Officer: OR 1.59 (0.41, 6.17) | ||||||
| [75] | M, F | [4], [5] | No significant difference in age-adjusted prevalence between the 3 job categories | |||
| [76] | M, F | Type of duty | School educator: 0.00%, fire-control: 0.67%, paramedics and rescue: 0.47%, office administrator: 1.08%, retirees: 2.63% | |||
| [77] | M, F | FF rank | Cadet/FF: 10.6%, engineer/driver/captain: 2.7%, officer, chief of staff: 7.2% | |||
| Post-traumatic stress disorder | ||||||
| [38] | M | [FF], [Administration] | [FF] | |||
| Senior fire sergeant: OR 1.28 (0.72, 2.28) | ||||||
| Fire sergeant: OR 2.28 (1.28, 4.06)* | ||||||
| Fire lieutenant: OR 2.47 (1.14, 5.37)* | ||||||
| Fire captain: OR 2.88 (1.11, 7.45)* | ||||||
| Fire chief: OR 2.11 (0.48, 9.28) | ||||||
| [Administration] | ||||||
| Firefighting: OR 2.04 (1.00, 4.17) | ||||||
| Rescue: OR 2.22 (0.84, 5.86) | ||||||
| EMS: OR 3.68 (1.47, 9.23)* | ||||||
| [55] | M, F | [Current FF] | Retired FF: unadjusted OR 2.61 (1.47, 4.64)* | |||
| [60] | M, F | [5] | HR 1.40 (1.26, 1.56)* | |||
| [62] | M | [Temporary FF] | Permanent FF: OR 0.30 (0.10, 0.90)* | |||
| [76] | M, F | Type of duty | School educator: 6.00%, fire-control: 10.94%, paramedics and rescue: 14.08%, office administrator: 9.19%, retirees: 11.84% | |||
| [79] | M, F | [2] | FF 4.56%*, [2] 1.73%* | |||
| [80] | M, F | [Group manager or higher] | FF/control operator: OR 1.50 (0.51, 4.40) | |||
| Crew manager: OR 1.75 (0.61, 4.99) | ||||||
| Watch manager: OR 1.69 (0.61, 4.65) | ||||||
| Station manager: OR 2.41 (0.87, 6.70) | ||||||
| Complex post-traumatic stress disorder | ||||||
| [80] | M, F | [Group manager or higher] | FF/control operator: OR 1.78 (1.01, 3.13)* | |||
| Crew manager: OR 1.45 (0.82, 2.57) | ||||||
| Watch manager: OR 1.08 (0.62, 1.89) | ||||||
| Station manager: OR 1.04 (0.56, 1.92) | ||||||
| Stress disorder | ||||||
| [75] | M, F | [4], [5] | No significant difference in age-adjusted prevalence between the 3 job categories | |||
| Excessive daytime sleepiness | ||||||
| [40] | M | Type of duty | On duty 13.7%, off-duty 14.0% | |||
| [81] | M, F | Volunteer FF | Professional FF: 38.2%*, volunteer FF: 23.5%* | |||
| Non-organic sleep disorders | ||||||
| [75] | M, F | [4], [5] | No significant difference in age-adjusted prevalence between the 3 job categories | |||
| (4) Nervous system diseases | ||||||
| [23] | M | [1] | SMR 0.73 (0.20, 1.88) | |||
| [26] | M | [1] | SMR 0.47 (0.27, 0.83)* | |||
| [29] | M | [1] | SMR 0.54 (0.31, 0.86)* | |||
| [47] | M | [1] | SMR 0.68 (0.46, 0.96)* | |||
| [65] | M | [2], [3] | [2] SMR 0.50 (0.32, 0.78)* | |||
| [3] SMR 0.76 (0.48, 1.19) | ||||||
| [72] | M, F | [1] | SMR 0.89 (0.80, 1.00) | |||
| Obstructive sleep apnea | ||||||
| [81] | M, F | Volunteer FF | Professional FF: 3.6%, volunteer FF: 0.7% | |||
| Sleep disorders | ||||||
| [43] | M | Tenure (yr) | ≥20 yr: 37.7%*, 10-20 yr: 51.3%*, <10 yr: 52.5%* | |||
| [60] | M, F | [5] | HR 1.04 (1.01, 1.08)* | |||
| [76] | M, F | Type of duty | School educator: 50.00%, fire-control: 53.79%, paramedics and rescue: 53.05%, office administrator: 56.22%, retirees: 36.84% | |||
| [81] | M, F | Volunteer FF | Professional FF: 37.5%*, volunteer FF: 22.6%* | |||
| Insomnia | ||||||
| [69] | M | [7] | FF 14.5%*, [7] 1.3%* | |||
| [74] | M, F | [Administrative] | Fire suppression: OR 2.45 (1.46, 4.12)* | |||
| EMS/rescue: OR 1.87 (1.10, 3.16)* | ||||||
| [81] | M, F | Volunteer FF | Professional FF: 19.9%, volunteer FF: 16.4% | |||
| Transient ischemic attack | ||||||
| [63] | M | [2] | SIR 1.12 (0.97, 1.30) | |||
| (5) Hearing impairment and deafness | ||||||
| Hearing loss | ||||||
| [28] | M | [1] | HF hearing loss: RR 2.9 (1.7, 5.1)* | |||
| Broad frequency hearing loss: RR 2.9 (1.5, 5.6)* | ||||||
| [30] | M | [8] | FF did not exhibit excessive loss of hearing compared with the comparison groups | |||
| [35] | M, F | Work period | 4,000 Hz mean (SD) | |||
| <5 yr: 9.6 (6.2)*, 5-9 yr: 12.0 (9.5)*, 10-14 yr: 15.1 (9.6)*, ≥15 yr: 27.9 (16.2)* | ||||||
| [41] | M, F | Yr in fire services | HF hearing loss: <5 yr: 5.0%*, 5-9 yr: 25.5%*, 10-19 yr: 32.2%*, 20-29 yr: 52.7%*, ≥30 yr: 74.4%* | |||
| LF hearing loss: <5 yr: 0.0%*, 5-9 yr: 0.0%*, 10-19 yr: 3.8%*, 20-29 yr: 10.9%*, ≥30 yr: 15.4%* | ||||||
| [46] | M | [9], [10] | [9] PR 5.29 (3.34, 8.39)*, [10] PR 0.99 (0.95, 1.03) | |||
| [10] Rescuer: PR 1.005 (1.002, 1.007)* | ||||||
| Paramedic: PR 1.001 (0.998, 1.005) | ||||||
| Suppressor: PR 0.999 (0.997, 1.000) | ||||||
| Office worker: PR 0.999 (0.997, 1.001) | ||||||
| [50] | M, F | [<10 yr] | 10-19 yr: OR 1.7 (0.6, 4.4) | |||
| ≥20 yr: OR 2.0 (0.6, 6.0) | ||||||
| [51] | M, F | [11] | HF hearing loss: FF 34.4%, [11] 58.7% | |||
| LF hearing loss: FF 3.9%, [11] 19.9% | ||||||
| Tinnitus | ||||||
| [51] | M, F | [10] | FF 40.3%, [11] 39.4% | |||
| (6) Circulatory diseases | ||||||
| [16] | M | [1] | SMR 0.86 | |||
| [18] | M | [1], [4] | [1] SMR 0.81 (0.73, 0.89)* | |||
| [4] SMR 0.83 | ||||||
| [4] IDR 0.91 (0.76, 1.09) | ||||||
| [29] | M, F | [1] | Male FF: SMR 0.69 (0.63, 0.76)* | |||
| Female FF: SMR 2.49 (1.32, 4.25)* | ||||||
| [45] | M | [1], [non-FF and employed <10 yr] | [1] SMR 0.27 (0.20, 0.37)* | |||
| [non-FF and employed <10 yr] | ||||||
| 10-20 yr: ARR 1.57 (0.72, 3.41) | ||||||
| ≥20 yr: ARR 1.40 (0.72, 2.74) | ||||||
| [47] | M | [1] | SMR 0.76 (0.68, 0.85)* | |||
| Heart disease | ||||||
| [20] | M | [1] | RR 0.89 (0.81, 0.97)2* | |||
| [21] | M | [4] | IDR 0.86 (0.74, 1.00) | |||
| [23] | M | [1] | SMR 1.10 (0.92, 1.31) | |||
| Rheumatic heart disease | ||||||
| [16] | M | [1] | SMR 0.29 | |||
| Hypertension | ||||||
| [37] | M, F | [2] | FF 26.7%, [2] 34.8% | |||
| [50] | M, F | [<10 yr] | 10-19 yr: OR 4.2 (1.3, 14.0)* | |||
| ≥20 yr: OR 5.0 (1.3, 20.2)* | ||||||
| [60] | M | [5] | HR 0.85 (0.82, 0.88)* | |||
| [65] | M, F | [2], [3] | [2] SMR 0.96 (0.54, 1.69) | |||
| [3] SMR 1.01 (0.57, 1.77) | ||||||
| [75] | M, F | [4], [5] | No significant difference in age-adjusted prevalence between the 3 job categories | |||
| Angina pectoris | ||||||
| [60] | M | [5] | HR 1.06 (1.02, 1.10)* | |||
| [63] | M, F | [2] | SIR 1.16 (1.08, 1.24)* | |||
| Myocardial infarction | ||||||
| [73] | M, F | [1] | HR 1.24 (1.07, 1.43)* | |||
| Acute myocardial infarction | ||||||
| [60] | M | [5] | HR 1.21 (1.10, 1.32)* | |||
| [63] | M | [2] | SIR 1.16 (1.06, 1.26)* | |||
| Ischemic heart disease | ||||||
| [19] | M | [2] | SMR 1.15 (0.74, 1.71) | |||
| [20] | M | [1] | RR 0.95 (0.87, 1.04)2 | |||
| [21] | M | [4] | IDR 0.88 (0.74, 1.04) | |||
| [23] | M | [1] | SMR 1.05 (0.86, 1.27) | |||
| [24] | M | [1] | SMR 0.74 (0.20, 1.90) | |||
| [26] | M | [1] | SMR 1.09 (1.02, 1.16)* | |||
| [45] | M | [1], [non-FF and employed <10 yr] | [1] SMR 0.42 (0.25, 0.66)* | |||
| [non-FF and employed <10 yr] | ||||||
| 10-20 yr: ARR 1.35 (0.44, 4.14) | ||||||
| ≥20 yr: ARR 0.93 (0.34, 2.51) | ||||||
| [61] | M, F | [1] | OR 0.98 (0.88, 1.10) | |||
| [65] | M | [2], [3] | [2] SMR 0.86 (0.73, 1.02) | |||
| [3] SMR 1.00 (0.84, 1.18) | ||||||
| [72] | M, F | [1] | SMR 0.98 (0.95, 1.01) | |||
| [75] | M, F | [4], [5] | No significant difference in age-adjusted prevalence between the 3 job categories | |||
| Chronic ischemic heart disease | ||||||
| [63] | M | [2] | SIR 1.15 (1.06, 1.24)* | |||
| Heart failure | ||||||
| [63] | M | [2] | SIR 1.01 (0.91, 1.12) | |||
| Sudden cardiac death | ||||||
| [42] | N.S. | [Non-emergency duties] | Fire suppression: RR 22.1 (14.8, 32.9)* | |||
| Alarm response: RR 2.6 (1.5, 4.6)* | ||||||
| Alarm return: RR 4.1 (2.7, 6.2)* | ||||||
| Atrial fibrillation/flutter | ||||||
| [63] | M | [2] | SIR 1.25 (1.14, 1.36)* | |||
| CHD | ||||||
| [31] | N.S. | [Non-emergency duties] | Fire suppression: RR 12.1-136.0* | |||
| Alarm response: RR 2.8-14.1* | ||||||
| Alarm return RR: 2.2-10.5* | ||||||
| [37] | M | [2] | FF CHD risk score 6.5% (SD 3.7)* | |||
| [2] CHD risk score 9.5% (SD 6.5)* | ||||||
| Cardiovascular diseases | ||||||
| [29] | M, F | [1] | Male FF: SMR 0.73 (0.65, 0.83)* | |||
| Female FF: SMR 3.85 (1.66, 7.58)* | ||||||
| [63] | M | [2] | SIR 1.10 (1.05, 1.15)* | |||
| Cerebrovascular diseases | ||||||
| [20] | M | [1] | RR 0.84 (0.67, 1.03)2 | |||
| [21] | M | [4] | IDR 0.65 (0.45, 0.92)* | |||
| [23] | M | [1] | SMR 0.38 (0.17, 0.73)* | |||
| [24] | M | [1] | SMR 1.16 (0.24, 3.38) | |||
| [26] | M | [1] | SMR 0.83 (0.69, 0.99)* | |||
| [45] | M | [1], [non-FF and employed <10 yr] | [1] SMR 0.24 (0.14, 0.38)* | |||
| [non-FF and employed <10 yr] | ||||||
| 10-20 yr: ARR 1.30 (0.31, 5.43) | ||||||
| ≥20 yr: ARR 1.87 (0.63, 5.59) | ||||||
| [60] | M, F | [5] | HR 0.97 (0.90 1.04) | |||
| [61] | M, F | [1] | OR 0.82 (0.67, 0.99)* | |||
| [65] | M | [2], [3] | [2] SMR 0.81 (0.61, 1.07) | |||
| [3] SMR 0.91 (0.69, 1.21) | ||||||
| [72] | M, F | [1] | SMR 0.90 (0.83, 0.97)* | |||
| [75] | M, F | [4], [5] | No significant difference in age-adjusted prevalence between the 3 job categories | |||
| Ischemic stroke | ||||||
| [73] | M, F | [1] | HR 1.43 (1.12, 1.82)* | |||
| Hemorrhagic stroke | ||||||
| [73] | M, F | [1] | HR 1.13 (0.74, 1.73) | |||
| Arteriosclerosis | ||||||
| [23] | M | [1] | SMR 1.49 (0.77, 2.61) | |||
| [63] | M | [2] | SIR 1.02 (0.88, 1.18) | |||
| (7) Respiratory diseases | ||||||
| [16] | M | [1] | SMR 0.93 | |||
| [18] | M | [1], [4] | [1] SMR 0.88 (0.66, 1.17) | |||
| [4] SMR 1.41 | ||||||
| [4] unadjusted IDR 1.98 (1.09, 3.87)* | ||||||
| [20] | M | [1] | RR 0.63 (0.40, 0.95)2* | |||
| [21] | M | [4] | IDR 1.11 (0.71, 1.73) | |||
| [26] | M | [1] | SMR 0.67 (0.55, 0.82)* | |||
| [29] | M, F | [1] | Male FF: SMR 0.50 (0.35, 0.70)* | |||
| Female FF: SMR 2.88 (0.58, 8.43) | ||||||
| [45] | M | [1], [non-FF and employed <10 yr] | [1] SMR 0.13 (0.03, 0.37)* | |||
| [non-FF and employed <10 yr] | ||||||
| ≥20 yr: ARR 5.89 (0.34, 101.13) | ||||||
| [47] | M | [1] | SMR 0.54 (0.39, 0.73)* | |||
| [72] | M, F | [1] | SMR 0.81 (0.76, 0.86)* | |||
| Acute respiratory infection | ||||||
| [20] | M | [1] | RR 0.63 (0.40, 0.95)2* | |||
| [65] | M | [2], [3] | [2] SMR 1.15 (0.16, 8.14) | |||
| [3] SMR 1.60 (0.23, 11.35) | ||||||
| Pneumonia | ||||||
| [21] | M | [4] | IDR 1.04 (0.46, 2.36) | |||
| [29] | M, F | [1] | Male FF: SMR 0.34 (0.17, 0.62)* | |||
| Female FF: SMR 4.35 (0.49, 15.70) | ||||||
| [65] | M | [2] [3] | [2] SMR 0.36 (0.16, 0.80)* | |||
| [3] SMR 0.48 (0.22, 1.07) | ||||||
| Bronchitis, emphysema and asthma | ||||||
| [65] | M | [2], [3] | [2] SMR 0.71 (0.52, 0.98)* | |||
| [3] SMR 0.94 (0.69, 1.30) | ||||||
| Asthma | ||||||
| [17] | M | Non-exposed FF | FF 9.4%, non-exposed FF 0.0% | |||
| [20] | M | [1] | RR 0.31 (0.01, 1.75)2 | |||
| [34] | M, F | [4] | FF 8.7%, [4] 7.2% | |||
| [50] | M, F | [<10 yr] | 10-19 yr: OR 1.4 (0.5, 3.5) | |||
| ≥20 yr: OR 2.0 (0.5, 8.3) | ||||||
| [64] | M | [3] | SIR 1.58 (1.32, 1.88)* | |||
| Bronchitis | ||||||
| [17] | M | Non-exposed FF | FF 14.3%, non-exposed FF 0.0% | |||
| Chronic bronchitis | ||||||
| [20] | M | [1] | RR 0.74 (0.15, 2.17)2 | |||
| [24] | M | [1] | SMR 1.83 (0.05, 10.21) | |||
| Emphysema | ||||||
| [20] | M | [1] | RR 0.52 (0.24, 0.99)2* | |||
| [21] | M | [4] | IDR 1.45 (0.54, 3.88) | |||
| [26] | M | [1] | SMR 0.64 (0.40, 1.02) | |||
| [29] | M, F | [1] | Male FF: SMR 0.87 (0.40, 1.66) | |||
| Female FF: SMR 12.5 (0.16, 69.60) | ||||||
| Chronic obstructive pulmonary disease | ||||||
| [20] | M | [1] | RR 0.75 (0.43, 1.23)2 | |||
| [21] | M | [4] | IDR 1.11 (0.65, 1.89) | |||
| [23] | M | [1] | SMR 1.57 (0.78, 2.81) | |||
| [64] | M | [3] | SIR 1.14 (0.98, 1.32) | |||
| [72] | M, F | [1] | SMR 0.78 (0.71, 0.85)* | |||
| (8) Digestive diseases | ||||||
| [16] | M | [1] | SMR 0.85 | |||
| [20] | M | [1] | RR 1.57 (1.27, 1.92)2* | |||
| [23] | M | [1] | SMR 0.46 (0.21, 0.89)* | |||
| [26] | M | [1] | SMR 0.97 (0.81, 1.17) | |||
| [29] | M, F | [1] | Male FF: SMR 0.57 (0.43, 0.73)* | |||
| Female FF: SMR 1.60 (0.18, 5.78) | ||||||
| [45] | M | [1], [non-FF and employed <10 yr] | [1] SMR 0.24 (0.16, 0.34) | |||
| [non-FF and employed <10 yr] | ||||||
| ≥20 yr: ARR 1.17 (0.40, 3.44) | ||||||
| [47] | M | [1] | SMR 0.79 (0.65, 0.95)* | |||
| Diseases of the stomach and duodenum | ||||||
| [20] | M | [1] | RR 1.57 (0.93, 2.49)2 | |||
| Diseases of the oral cavity, esophagus and stomach | ||||||
| [65] | M | [2], [3] | [2] SMR 0.43 (0.16, 1.15) | |||
| Gastric and duodenal ulcers | [3] SMR 0.60 (0.22, 1.59) | |||||
| [26] | M | [1] | SMR 0.67 (0.38, 1.17) | |||
| Peptic ulcer disease | ||||||
| [60] | M, F | [5] | HR 1.13 (1.11, 1.15)* | |||
| [67] | M | [4] | Self-reported PUD: FF 7.1%*, [4] 8.3%* | |||
| Self-reports of physician-diagnosed PUD: FF 5.5%*, [4] 6.5%* | ||||||
| Hernia and intestinal obstruction | ||||||
| [20] | M | [1] | RR 0.64 (0.13, 1.89)2 | |||
| Liver diseases | ||||||
| [45] | M | [1], [non-FF and employed <10 yr] | [1] SMR 0.26 (0.17, 0.37)* | |||
| [non-FF and employed <10 yr] | ||||||
| ≥20 yr: ARR 1.42 (0.46, 4.38) | ||||||
| Alcoholic liver disease | ||||||
| [60] | M, F | [5] | HR 0.80 (0.76, 0.83)* | |||
| Cirrhosis and chronic liver disease | ||||||
| [20] | M | [1] | RR 2.27 (1.73, 2.93)2* | |||
| [26] | M | [1] | SMR 1.10 (0.84, 1.43) | |||
| [72] | M, F | [1] | SMR 1.16 (1.03, 1.29) | |||
| Diseases of the liver and bile duct | ||||||
| [65] | M | [2], [3] | [2] SMR 0.73 (0.54, 0.98)* | |||
| [3] SMR 0.85 (0.63, 1.15) | ||||||
| (9) Musculoskeletal system diseases | ||||||
| [47] | M | [1] | SMR 0.00 (0.00, 0.58)* | |||
| [75] | M, F | [4], [5] | No significant difference in age-adjusted prevalence between the 3 job categories | |||
| Non-rheumatoid arthritis | ||||||
| [50] | M, F | [<10 yr] | 10-19 yr: OR 2.0 (0.7, 6.4) | |||
| ≥20 yr: OR 1.5 (0.4, 5.8) | ||||||
| Facet joint degeneration | ||||||
| [56] | M | [7] | L1-L2: OR 2.64 (1.31, 5.31)* | |||
| L2-L3: OR 2.28 (1.30, 4.00)* | ||||||
| L3-L4: OR 1.41 (0.81, 2.46) | ||||||
| L4-L5: OR 1.91 (1.03, 3.54)* | ||||||
| L5-S1: OR 1.81 (1.03, 3.18)* | ||||||
| Spinal stenosis | ||||||
| [69] | M | [7] | FF 33.0%, [7] 20.8%* | |||
| Lumbar disc herniation | ||||||
| [53] | M, F | [Administrative] | L1-L2 intervertebral disc: OR 1.19 (0.44, 3.22) | |||
| L2-L3 intervertebral disc: OR 1.33 (0.50, 3.55) | ||||||
| L3-L4 intervertebral disc: OR 1.73 (0.48, 6.22) | ||||||
| L4-L5 intervertebral disc: OR 3.49 (1.24, 9.86)* | ||||||
| L5-S1 intervertebral disc: OR 1.18 (0.47, 2.96) | ||||||
| [60] | M, F | [5] | HR 1.43 (1.39, 1.46)* | |||
| [69] | M | [7] | FF 51.9%*, [7] 36.4%* | |||
| LBP | ||||||
| [48] | M | Yr in fire services | During the 13 yr follow-up, the prevalence of radiating LBP increased from 16 to 29% and that of local LBP from 28 to 40%* | |||
| [58] | M | Duration of each job (yr) | LBP increased according to the increment of duration of EMS and ER work* | |||
| [60] | M, F | [5] | HR 1.52 (1.43, 1.63)* | |||
| [69] | M | [7] | EMS: OR 2.57 (1.20, 5.58)* | |||
| Rescue: OR 3.69 (1.37, 9.94)* | ||||||
| Job-related injuries | ||||||
| [36] | M, F | [<17 yr] | ≥17 yr: OR 2.96 (1.92, 4.58)* | |||
| [52] | M | [Officer] | Fire suppression: OR 1.86 (1.61, 2.15)* | |||
| EMS: OR 2.93 (2.51, 3.42)* | ||||||
| [59] | M, F | Primary position | Primary position was not significantly associated with work related injury | |||
| [66] | N.S | [Career FF] | Volunteer burns: OR 1.7 (1.2, 2.4)* | |||
| Volunteer trauma: OR 1.8 (1.5, 2.2)* | ||||||
| (10) Genitourinary diseases | ||||||
| [16] | M | [1] | SMR 0.49 | |||
| [23] | M | [1] | SMR 1.32 (0.57, 2.60) | |||
| [26] | M | [1] | SMR 0.54 (0.36, 0.81)* | |||
| [29] | M | [1] | SMR 0.38 (0.14, 0.83)* | |||
| [47] | M | [1] | SMR 0.94 (0.50, 1.61) | |||
| Chronic nephritis | ||||||
| [16] | M | [1] | SMR 0.38 | |||
| Nephritis and kidney stones | ||||||
| [65] | M | [2], [3] | [2] SMR 0.67 (0.10, 4.79) | |||
| [3] SMR 1.06 (0.15, 7.56) | ||||||
| Male infertility | ||||||
| [70] | M | [2], [3] | Male In Vitro Fertilization model: [2] HR 1.46 (1.10, 1.94)*, [3] HR 1.40 (1.06, 1.86)* | |||
| Male National Patient Register model: [2] HR 1.53 (1.18, 1.98)*, [3] HR 1.36 (1.05, 1.75)* | ||||||
| (11) Suicidal behavior | ||||||
| Suicide | ||||||
| [16] | M | [1] | SMR 0.19 | |||
| [23] | M | [1] | SMR 0.38 (0.15, 0.79)* | |||
| [24] | M | [1] | SMR 0.47 (0.06, 1.69) | |||
| [26] | M | [1] | SMR 0.66 (0.48, 0.92)* | |||
| [29] | M, F | [1] | Male FF: SMR 0.55 (0.44, 0.68)* | |||
| Female FF: SMR 2.52 (0.68, 6.44) | ||||||
| [49] | M | [1] | FF 11.61 per 100,000 PY, [1] 18.53 per 100,000 PY | |||
| [65] | M | [2], [3] | [2] SMR 0.65 (0.48, 0.87)* | |||
| [3] SMR 0.78 (0.57, 1.05) | ||||||
| [78] | M, F | [2] | PMR 1.72 (1.53, 1.93)* | |||
| [44] | M, F | [Lower rank], length of service | [Lower rank] | |||
| Higher rank: OR 1.04 (0.72, 1.51) | ||||||
| Officer rank: OR 0.14 (0.06, 0.35)* | ||||||
| FF with fewer yr of service were more likely to report suicide attempts (b=-0.14)* | ||||||
| Suicide attempt | ||||||
| [79] | M, F | [2] | FF 24.21%*, [2] 33.39%* | |||
| Suicidal ideation | ||||||
| [44] | M, F | [Lower rank], length of service | [Lower rank] | |||
| Higher rank: OR 0.97 (0.73, 1.30) | ||||||
| Officer rank: OR 0.64 (0.44, 0.92)* | ||||||
| FF with fewer yr of service were more likely to report career suicidal ideation (b=-0.03)* | ||||||
| [68] | M, F | [Fire suppression] | EMS: OR 0.76 (0.70, 0.82)* | |||
| Officers: OR 1.48 (1.36, 1.62)* | ||||||
| Suicide plan | ||||||
| [44] | M, F | [Lower rank], length of service | [Lower rank] | |||
| Higher rank: OR 0.77 (0.54, 1.10) | ||||||
| Officer rank: OR 0.33 (0.19, 0.59)* | ||||||
| FF with fewer yr of service were more likely to report suicide plans (b=-0.08)* | ||||||
| Non-suicidal self-injury | ||||||
| [44] | M, F | [Lower rank], length of service | [Lower rank] | |||
| Higher rank: OR 0.93 (0.65, 1.34) | ||||||
| Officer rank: OR 0.10 (0.03, 0.27)* | ||||||
| FF with fewer yr of service were more likely to report non-suicidal self-injury (b=-0.15)* | ||||||
| Intentional self-harm | ||||||
| [45] | M, F | [1], [non-FF and employed <10 yr] | [1] SMR 0.45 (0.33, 0.60)* | |||
| [non-FF and employed <10 yr] | ||||||
| 10-20 yr: ARR 0.56 (0.28, 1.12) | ||||||
| ≥20 yr: ARR 2.57 (1.01, 6.64)* | ||||||
| (12) Other diseases | ||||||
| Circulatory congenital malformations | ||||||
| [65] | M | [2], [3] | [2] SMR 2.35 (0.76, 7.28) | |||
| [3] SMR 6.95 (2.24, 21.54)* | ||||||
| Sarcoidosis | ||||||
| [25] | M | EMS Prehospital health-care workers | FF | |||
| Annual incidence proportions: 12.9/100,000 | ||||||
| Point prevalence: 222/100,000 | ||||||
| EMS prehospital health-care workers | ||||||
| Annual incidence proportions: 0 | ||||||
| Point prevalence: 35/100,000 | ||||||
| Atopy | ||||||
| [32] | M | [1], duration of employment | FF 51%*, [1] 32%* | |||
| Duration of employment did not account for the differences in prevalence of atopy | ||||||
| Burnout | ||||||
| [67] | M | [4] | FF 24.2%*, [4] 22.5%* | |||
In this study, the criterion for the SMR, IDR, or PMR was 1; In studies that reported results by multiplying the SMR, IDR, or PMR by 100, the corresponding result was divided by 100 and organized in a table.
RN, reference number; M, male; F, female; N.S., not specified; CI, confidence interval; RR, relative risk; ARR, adjusted relative risk; SMR, standardized mortality ratio; SIR, standardized incidence ratio; HR, hazard ratio; OR, odds ratio; PR, prevalence ratio; IDR, incidence density ratio; PMR, proportionate mortality ratio; EMS, emergency medical service; ER, emergency rescue; FF, firefighters; HF, high frequency; LF, low frequency; PY, person years; LBP, lower back pain; SD, standard deviation; PUD, peptic ulcer disease; CHD, coronary heart disease.
1 The numbers and words in [ ] of the comparison indicate the reference category of the study; The comparison groups are denoted as follows: [1], general population; [2], employees; [3], military employees; [4], police officers; [5], national and regional government officer; [6], office workers; [7], hospital office workers; [8], non–occupationally exposed groups of individuals; [9], otologically normal male Korean population; [10], non-industrial noise-exposed male Korean population.
2 In this study, rate ratio (RR): where 1.00 indicates an equal number of observed and expected events.
* p<0.05.
- 1. Guidotti TL. Occupational mortality among firefighters: assessing the association. J Occup Environ Med 1995;37:1348-1356.PubMed
- 2. Groot E, Caturay A, Khan Y, Copes R. A systematic review of the health impacts of occupational exposure to wildland fires. Int J Occup Med Environ Health 2019;32:121-140.ArticlePubMed
- 3. Aronson KJ, Tomlinson GA, Smith L. Mortality among fire fighters in metropolitan Toronto. Am J Ind Med 1994;26:89-101.ArticlePubMed
- 4. Vena JE, Fiedler RC. Mortality of a municipal-worker cohort: IV. Fire fighters. Am J Ind Med 1987;11:671-684.ArticlePubMed
- 5. Howe GR, Burch JD. Fire fighters and risk of cancer: an assessment and overview of the epidemiologic evidence. Am J Epidemiol 1990;132:1039-1050.ArticlePubMed
- 6. Casjens S, Brüning T, Taeger D. Cancer risks of firefighters: a systematic review and meta-analysis of secular trends and regionspecific differences. Int Arch Occup Environ Health 2020;93:839-852.ArticlePubMedPMCPDF
- 7. Tornling G, Gustavsson P, Hogstedt C. Mortality and cancer incidence in Stockholm fire fighters. Am J Ind Med 1994;25:219-228.ArticlePubMed
- 8. Kang D, Davis LK, Hunt P, Kriebel D. Cancer incidence among male Massachusetts firefighters, 1987-2003. Am J Ind Med 2008;51:329-335.ArticlePubMed
- 9. Laroche E, L’Espérance S. Cancer incidence and mortality among firefighters: an overview of epidemiologic systematic reviews. Int J Environ Res Public Health 2021;18:2519.PubMedPMC
- 10. Daniels RD, Kubale TL, Yiin JH, Dahm MM, Hales TR, Baris D, et al. Mortality and cancer incidence in a pooled cohort of US firefighters from San Francisco, Chicago and Philadelphia (1950-2009). Occup Environ Med 2014;71:388-397.ArticlePubMedPMC
- 11. LeMasters GK, Genaidy AM, Succop P, Deddens J, Sobeih T, Barriera-Viruet H, et al. Cancer risk among firefighters: a review and meta-analysis of 32 studies. J Occup Environ Med 2006;48:1189-1202.ArticlePubMed
- 12. International Agency for Research on Cancer (IARC). IARC monographs on the evaluation of carcinogenic risks to humans, vol 98: painting, firefighting, and shiftwork; 2010 [cited 2022 Aug 1]. Available from: https://monographs.iarc.who.int/wp-content/uploads/2018/06/mono98.pdf.
- 13. Crawford JO, Graveling RA. Non-cancer occupational health risks in firefighters. Occup Med (Lond) 2012;62:485-495.ArticlePubMed
- 14. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ 2009;339:b2700.ArticlePubMedPMC
- 15. Kim SY, Seo HJ, Lee YJ, Park JE. Study design algorithm for medical literature of intervention (DAMI) and risk of bias for nonrandomized studies (RoBANS) ver. 2.0 by HIRA. Seoul: Health Insurance Review & Assessment Service; 2013. p 65-66 (Korean).
- 16. Musk AW, Monson RR, Peters JM, Peters RK. Mortality among Boston firefighters, 1915--1975. Br J Ind Med 1978;35:104-108.ArticlePubMedPMC
- 17. Markowitz JS. Self-reported short- and long-term respiratory effects among PVC-exposed firefighters. Arch Environ Health 1989;44:30-33.ArticlePubMed
- 18. Rosénstock L, Demers P, Heyer NJ, Barnhart S. Respiratory mortality among firefighters. Br J Ind Med 1990;47:462-465.ArticlePubMedPMC
- 19. Hansen ES. A cohort study on the mortality of firefighters. Br J Ind Med 1990;47:805-809.ArticlePubMedPMC
- 20. Beaumont JJ, Chu GS, Jones JR, Schenker MB, Singleton JA, Piantanida LG, et al. An epidemiologic study of cancer and other causes of mortality in San Francisco firefighters. Am J Ind Med 1991;19:357-372.ArticlePubMed
- 21. Demers PA, Heyer NJ, Rosenstock L. Mortality among firefighters from three northwestern United States cities. Br J Ind Med 1992;49:664-670.ArticlePubMedPMC
- 22. Woodruff BA, Moyer LA, O’Rourke KM, Margolis HS. Blood exposure and the risk of hepatitis B virus infection in firefighters. J Occup Med 1993;35:1048-1054.PubMed
- 23. Guidotti TL. Mortality of urban firefighters in Alberta, 1927-1987. Am J Ind Med 1993;23:921-940.ArticlePubMed
- 24. Deschamps S, Momas I, Festy B. Mortality amongst Paris fire-fighters. Eur J Epidemiol 1995;11:643-646.ArticlePubMedPDF
- 25. Prezant DJ, Dhala A, Goldstein A, Janus D, Ortiz F, Aldrich TK, et al. The incidence, prevalence, and severity of sarcoidosis in New York City firefighters. Chest 1999;116:1183-1193.ArticlePubMed
- 26. Baris D, Garrity TJ, Telles JL, Heineman EF, Olshan A, Zahm SH. Cohort mortality study of Philadelphia firefighters. Am J Ind Med 2001;39:463-476.ArticlePubMed
- 27. Upfal MJ, Naylor P, Mutchnick MM. Hepatitis C screening and prevalence among urban public safety workers. J Occup Environ Med 2001;43:402-411.ArticlePubMed
- 28. Kales SN, Freyman RL, Hill JM, Polyhronopoulos GN, Aldrich JM, Christiani DC. Firefighters’ hearing: a comparison with population databases from the International Standards Organization. J Occup Environ Med 2001;43:650-656.ArticlePubMed
- 29. Ma F, Fleming LE, Lee DJ, Trapido E, Gerace TA, Lai H, et al. Mortality in Florida professional firefighters, 1972 to 1999. Am J Ind Med 2005;47:509-517.ArticlePubMed
- 30. Clark WW, Bohl CD. Hearing levels of firefighters: risk of occupational noise-induced hearing loss assessed by cross-sectional and longitudinal data. Ear Hear 2005;26:327-340.ArticlePubMed
- 31. Kales SN, Soteriades ES, Christophi CA, Christiani DC. Emergency duties and deaths from heart disease among firefighters in the United States. N Engl J Med 2007;356:1207-1215.ArticlePubMed
- 32. Miedinger D, Chhajed PN, Stolz D, Gysin C, Wanzenried AB, Schindler C, et al. Respiratory symptoms, atopy and bronchial hyperreactivity in professional firefighters. Eur Respir J 2007;30:538-544.ArticlePubMed
- 33. Saijo Y, Ueno T, Hashimoto Y. Twenty-four-hour shift work, depressive symptoms, and job dissatisfaction among Japanese firefighters. Am J Ind Med 2008;51:380-391.ArticlePubMed
- 34. Ribeiro M, de Paula Santos U, Bussacos MA, Terra-Filho M. Prevalence and risk of asthma symptoms among firefighters in São Paulo, Brazil: a population-based study. Am J Ind Med 2009;52:261-269.ArticlePubMed
- 35. Kim MG, Park SJ, Lee K, Lee DW, Kim KS, Lim HS. A study on the possibility of occupational noise-induced hearing loss in firefighters. Korean J Audiol 2011;15:62-66.
- 36. Hong O, Chin DL, Phelps S, Feld J, Vogel S. Occupational injuries, duty status, and factors associated with injuries among firefighters. Workplace Health Saf 2012;60:517-523.ArticlePubMed
- 37. Mochtar I, Hooper RW. Assessment of the 10-year risk of coronary heart disease events for Qatar Petroleum’s firefighters and non-firefighter staff in Qatar. East Mediterr Health J 2012;18:127-131.ArticlePubMed
- 38. Shin DY, Jeon MJ, Sakong J. Posttraumatic stress disorder and related factors in male firefighters in a metropolitan city. Korean J Occup Environ Med 2012;24:397-409 (Korean).ArticlePDF
- 39. Contrera-Moreno L, de Andrade SM, Pontes ER, Stief AC, Pompilio MA, Motta-Castro AR. Hepatitis B virus infection in a population exposed to occupational hazards: firefighters of a metropolitan region in central Brazil. Rev Soc Bras Med Trop 2012;45:463-467.ArticlePubMed
- 40. Haddock CK, Poston WS, Jitnarin N, Jahnke SA. Excessive daytime sleepiness in firefighters in the central United States. J Occup Environ Med 2013;55:416-423.ArticlePubMed
- 41. Hong O, Chin DL, Samo DG. Hearing loss and use of hearing protection among career firefighters in the United States. J Occup Environ Med 2013;55:960-965.ArticlePubMed
- 42. Farioli A, Yang J, Teehan D, Baur DM, Smith DL, Kales SN. Duty-related risk of sudden cardiac death among young US firefighters. Occup Med (Lond) 2014;64:428-435.ArticlePubMedPMC
- 43. Lim DK, Baek KO, Chung IS, Lee MY. Factors related to sleep disorders among male firefighters. Ann Occup Environ Med 2014;26:11.ArticlePubMedPMCPDF
- 44. Stanley IH, Hom MA, Hagan CR, Joiner TE. Career prevalence and correlates of suicidal thoughts and behaviors among firefighters. J Affect Disord 2015;187:163-171.ArticlePubMed
- 45. Ahn YS, Jeong KS. Mortality due to malignant and non-malignant diseases in Korean professional emergency responders. PLoS One 2015;10:e0120305.ArticlePubMedPMC
- 46. Kang TS, Hong OS, Kim KS, Yoon CS. Hearing among male firefighters: a comparison with hearing data from screened and unscreened male population. J Expo Sci Environ Epidemiol 2015;25:106-112.ArticlePubMedPMCPDF
- 47. Amadeo B, Marchand JL, Moisan F, Donnadieu S, Gaëlle C, Simone MP, et al. French firefighter mortality: analysis over a 30-year period. Am J Ind Med 2015;58:437-443.ArticlePubMed
- 48. Lusa S, Miranda H, Luukkonen R, Punakallio A. Sleep disturbances predict long-term changes in low back pain among Finnish firefighters: 13-year follow-up study. Int Arch Occup Environ Health 2015;88:369-379.ArticlePubMedPMCPDF
- 49. Stanley IH, Hom MA, Joiner TE. Suicide mortality among firefighters: results from a large, urban fire department. Am J Ind Med 2016;59:942-947.ArticlePubMed
- 50. Semmens EO, Domitrovich J, Conway K, Noonan CW. A cross-sectional survey of occupational history as a wildland firefighter and health. Am J Ind Med 2016;59:330-335.ArticlePubMed
- 51. Hong O, Chin DL, Phelps S, Joo Y. Double jeopardy: hearing loss and tinnitus among noise-exposed workers. Workplace Health Saf 2016;64:235-242.ArticlePubMedPDF
- 52. Yoon JH, Kim YK, Kim KS, Ahn YS. Characteristics of workplace injuries among nineteen thousand Korean firefighters. J Korean Med Sci 2016;31:1546-1552.ArticlePubMedPMCPDF
- 53. Jang TW, Ahn YS, Byun J, Lee JI, Kim KH, Kim Y, et al. Lumbar intervertebral disc degeneration and related factors in Korean firefighters. BMJ Open 2016;6:e011587.ArticlePubMedPMC
- 54. Strauß M, Foshag P, Przybylek B, Horlitz M, Lucia A, SanchisGomar F, et al. Occupation and metabolic syndrome: is there correlation? A cross sectional study in different work activity occupations of German firefighters and office workers. Diabetol Metab Syndr 2016;8:57.ArticlePubMedPMC
- 55. Harvey SB, Milligan-Saville JS, Paterson HM, Harkness EL, Marsh AM, Dobson M, et al. The mental health of fire-fighters: an examination of the impact of repeated trauma exposure. Aust N Z J Psychiatry 2016;50:649-658.ArticlePubMedPDF
- 56. Kim DH, An YS, Kim HD, Jeong KS, Ahn YS, Kim KH, et al. Comparison of facet joint degeneration in firefighters and hospital office workers. Ann Occup Environ Med 2017;29:24.ArticlePubMedPMCPDF
- 57. Lee W, Kim J. Prevalence of metabolic syndrome and related factors in Korean career firefighters in comparisons with other occupational groups. J Occup Environ Med 2017;59:384-388.ArticlePubMed
- 58. Kim MG, Seo JI, Kim K, Ahn YS. Nationwide firefighter survey: the prevalence of lower back pain and its related psychological factors among Korean firefighters. Int J Occup Saf Ergon 2017;23:447-456.ArticlePubMed
- 59. Phelps SM, Drew-Nord DC, Neitzel RL, Wallhagen MI, Bates MN, Hong OS. Characteristics and predictors of occupational injury among career firefighters. Workplace Health Saf 2018;66:291-301.ArticlePubMedPMCPDF
- 60. Han M, Park S, Park JH, Hwang SS, Kim I. Do police officers and firefighters have a higher risk of disease than other public officers? A 13-year nationwide cohort study in South Korea. BMJ Open 2018;8:e019987.ArticlePubMedPMC
- 61. Muegge CM, Zollinger TW, Song Y, Wessel J, Monahan PO, Moffatt SM. Excess mortality among Indiana firefighters, 1985-2013. Am J Ind Med 2018;61:961-967.ArticlePubMedPDF
- 62. Psarros C, Theleritis C, Kokras N, Lyrakos D, Koborozos A, Kakabakou O, et al. Personality characteristics and individual factors associated with PTSD in firefighters one month after extended wildfires. Nord J Psychiatry 2018;72:17-23.ArticlePubMed
- 63. Pedersen JE, Ugelvig Petersen K, Ebbehøj NE, Bonde JP, Hansen J. Incidence of cardiovascular disease in a historical cohort of Danish firefighters. Occup Environ Med 2018;75:337-343.ArticlePubMed
- 64. Pedersen JE, Ugelvig Petersen K, Ebbehøj NE, Bonde JP, Hansen J. Risk of asthma and chronic obstructive pulmonary disease in a large historical cohort of Danish firefighters. Occup Environ Med 2018;75:871-876.ArticlePubMed
- 65. Petersen KU, Pedersen JE, Bonde JP, Ebbehøj NE, Hansen J. Mortality in a cohort of Danish firefighters; 1970-2014. Int Arch Occup Environ Health 2018;91:759-766.ArticlePubMedPDF
- 66. Kahn SA, Leonard C, Siordia C. Firefighter fatalities: crude mortality rates and risk factors for line of duty injury and death. J Burn Care Res 2019;40:196-201.ArticlePubMed
- 67. Lin PY, Wang JY, Shih DP, Kuo HW, Liang WM. The interaction effects of burnout and job support on peptic ulcer disease (PUD) among firefighters and policemen. Int J Environ Res Public Health 2019;16:2369.ArticlePubMedPMC
- 68. Park H, Kim JI, Min B, Oh S, Kim JH. Prevalence and correlates of suicidal ideation in Korean firefighters: a nationwide study. BMC Psychiatry 2019;19:428.ArticlePubMedPMCPDF
- 69. Kim MG, Ahn YS. Associations between lower back pain and job types in South Korean male firefighters. Int J Occup Saf Ergon 2021;27:570-577.ArticlePubMed
- 70. Petersen KU, Hansen J, Ebbehoej NE, Bonde JP. Infertility in a cohort of male Danish firefighters: a register-based study. Am J Epidemiol 2019;188:339-346.ArticlePubMed
- 71. Azevedo DS, Lima EP, Gunn V, Muntaner C, Ng E, Assunção AA. Anxiety and contradictory class position in the hierarchy of Brazilian firefighters. Am J Ind Med 2019;62:1007-1013.ArticlePubMedPDF
- 72. Pinkerton L, Bertke SJ, Yiin J, Dahm M, Kubale T, Hales T, et al. Mortality in a cohort of US firefighters from San Francisco, Chicago and Philadelphia: an update. Occup Environ Med 2020;77:84-93.ArticlePubMedPMC
- 73. Noh J, Lee CJ, Hyun DS, Kim W, Kim MJ, Park KS, et al. Blood pressure and the risk of major adverse cardiovascular events among firefighters. J Hypertens 2020;38:850-857.ArticlePubMed
- 74. Jang TW, Jeong KS, Ahn YS, Choi KS. The relationship between the pattern of shift work and sleep disturbances in Korean firefighters. Int Arch Occup Environ Health 2020;93:391-398.ArticlePubMedPMCPDF
- 75. Min J, Kim Y, Kim HS, Han J, Kim I, Song J, et al. Descriptive analysis of prevalence and medical expenses of cancer, cardio-cerebrovascular disease, psychiatric disease, and musculoskeletal disease in Korean firefighters. Ann Occup Environ Med 2020;32:e7.ArticlePubMedPMCPDF
- 76. Kim YT, Kim WJ, Choi JE, Bae MJ, Jang H, Lee CJ, et al. Cohort profile: Firefighter Research on the Enhancement of Safety and Health (FRESH), a prospective cohort study on Korean firefighters. Yonsei Med J 2020;61:103-109.ArticlePubMedPMCPDF
- 77. Chen X, Zhang L, Peng Z, Chen S. Factors influencing the mental health of firefighters in Shantou City, China. Psychol Res Behav Manag 2020;13:529-536.PubMedPMC
- 78. Vigil NH, Beger S, Gochenour KS, Frazier WH, Vadeboncoeur TF, Bobrow BJ. Suicide among the emergency medical systems occupation in the United States. West J Emerg Med 2021;22:326-332.ArticlePubMedPMC
- 79. Pennington ML, Ylitalo KR, Lanning BA, Dolan SL, Gulliver SB. An epidemiologic study of suicide among firefighters: findings from the National Violent Death Reporting System, 2003-2017. Psychiatry Res 2021;295:113594.ArticlePubMed
- 80. Langtry J, Owczarek M, McAteer D, Taggart L, Gleeson C, Walshe C, et al. Predictors of PTSD and CPTSD in UK firefighters. Eur J Psychotraumatol 2021;12:1849524.ArticlePubMedPMC
- 81. Savall A, Marcoux P, Charles R, Trombert B, Roche F, Berger M. Sleep quality and sleep disturbances among volunteer and professional French firefighters: FIRESLEEP study. Sleep Med 2021;80:228-235.ArticlePubMed
- 82. Smith E, Holmes L, Larkin B. Health trends among 9/11 responders from 2011-2021: a review of World Trade Center Health Program statistics. Prehosp Disaster Med 2021;36:621-626.ArticlePubMed
- 83. Burgess JL, Witten ML, Nanson CJ, Hysong TA, Sherrill DL, Quan SF, et al. Serum pneumoproteins: a cross-sectional comparison of firefighters and police. Am J Ind Med 2003;44:246-253.ArticlePubMed
- 84. Kim DS, Moon MK, Kim KS. A survey of musculoskeletal symptoms & risk factors for the 119 emergency medical services (EMS) activities. J Ergon Soc Korea 2010;29:211-216 (Korean).Article
- 85. Agnew J, McDiarmid MA, Lees PS, Duffy R. Reproductive hazards of fire fighting. I. Non-chemical hazards. Am J Ind Med 1991;19:433-445.ArticlePubMed
- 86. Van Eerd D, Irvin E, Harbin S, Mahood Q, Tiong M. Occupational exposure and post-traumatic stress disorder: a rapid review. Work 2021;68:721-731.ArticlePubMed
- 87. Guidotti TL. Human factors in firefighting: ergonomic-, cardiopulmonary-, and psychogenic stress-related issues. Int Arch Occup Environ Health 1992;64:1-12.ArticlePubMedPDF
- 88. Thoits PA. Multiple identities and psychological well-being: a reformulation and test of the social isolation hypothesis. Am Sociol Rev 1983;48:174-187.ArticlePubMed
- 89. National Institute for Occupational Safety and Health (NIOSH). National firefighter registry: understanding and reducing cancer; 2019 [cited 2021 Dec 10]. Available from: https://www.cdc.gov/niosh/firefighters/registry.html.
REFERENCES
Figure & Data
References
Citations
- Associations between Recognition and Behaviors Regarding the Use, Washing and Management of Firefighting Protection Suits and Public Health Awareness of Occupational Exposure Risks among Firefighters
Soo Jin Kim, Seunghon Ham
Fire.2024; 7(5): 156. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite