Articles
- Page Path
- HOME > Epidemiol Health > Volume 43; 2021 > Article
-
Systematic Review
Prevalence of high-risk HPV genotypes in sub-Saharan Africa according to HIV status: a 20-year systematic review -
Jude Ogechukwu Okoye1
 , Chukwudi Amaechi Ofodile1, Oluwaseun Kelechi Adeleke2, Okechi Obioma3
, Chukwudi Amaechi Ofodile1, Oluwaseun Kelechi Adeleke2, Okechi Obioma3 -
Epidemiol Health 2021;43:e2021039.
DOI: https://doi.org/10.4178/epih.e2021039
Published online: May 25, 2021
1Department of Medical Laboratory Science, Faculty of Health Sciences and Technology, Nnamdi Azikiwe University, Nnewi, Nigeria
2Department of Medical Laboratory Science, Afe Babalola University, Ado Ekiti, Nigeria
3Department of Medical Laboratory Science, Abia State University, Uturu, Nigeria
- Correspondence: Jude Ogechukwu Okoye Department of Medical Laboratory Science, Faculty of Health Sciences and Technology, Nnamdi Azikiwe University, Nnewi Campus, Anambra State, Nigeria E-mail: jog.okoye@unizik.edu.ng
©2021, Korean Society of Epidemiology
This is an open-access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
OBJECTIVES
- This review assessed the rate of high-risk human papillomavirus (HPV) infection among women living in sub-Saharan Africa. It also determined the prevalence of high-risk HPV (hrHPV) among human immunodeficiency virus (HIV) seropositive (HIV+) and seronegative (HIV-) women in sub-Saharan Africa, pre-2010 and post-2010.
-
METHODS
- In this systematic review, Google Scholar, PubMed Central, and Embase were searched to identify cohort and case-control studies that investigated the relationship between HIV and HPV infection. The database searches yielded 17 studies published between 1999 and 2018.
-
RESULTS
- In the general population, the prevalence of any HPV/multiple HPV infections was higher among HIV+ (53.6/22.6%) than among HIV- women (26.5/7.3%) with odds ratios of 3.22 and 3.71, respectively (95% confidence interval, 3.00 to 3.42 and 2.39 to 5.75, p<0.001). The prevalent HPV genotypes among HIV+ and HIV- women diagnosed with invasive cervical cancer (ICC) were HPV-16/18 and HPV-45. The prevalence of HPV-16, HPV-18, and HPV-45 was lower in 1999-2010 (3.8, 1.7, and 0.8%, respectively) than in 2011-2018 (19.1, 6.0, and 3.6%, respectively). Among women diagnosed with ICC, HIV+ women had a higher prevalence of HPV-56, HPV-31, and HPV-51 (7.3, 5.3, and 3.3%, respectively) than HIV- women (1.3, 2.2, and 0.4%, p<0.001, p=0.050, and p=0.013, respectively).
-
CONCLUSIONS
- The prevalence of HPV infection, multiple HPV infections, and non-vaccine HPV types were higher among HIV+ women than among HIV- women in sub-Saharan Africa. Although HIV infection influences the distribution of HPV types, this study suggests that cervical cancer incidence in sub-Saharan Africa is primarily driven by the prevalence of vaccine hrHPVs, especially HPV-16 and HPV-18.
- Globally, cervical cancer is the third most common and deadly cancer among women [1]. The incidence of cervical cancer varies by race and region. According to the GLOBOCAN 2018 estimates, the mean age-standardized incidence rates (ASIR) for cervical cancer in sub-Saharan Africa and Northern Africa were 34.9 and 7.2, respectively [1,2]. This suggests that the ASIR of cervical cancer is higher in sub-Saharan Africa than in North Africa. Up to 2016, Jedy-Agba et al. [3] reported an increased incidence of cervical cancer in sub-Saharan Africa. The reason for the increasing incidence of cervical cancer in sub-Saharan Africa is still unknown. It could be related to the prevalence of human immunodeficiency virus (HIV) and human papillomavirus (HPV). In 2019, according to the Joint United Nations Program on HIV/AIDS, the population of people living with HIV in sub-Sahara Africa and Northern Africa was 12.9 million (3.9 to 23.0 million) and 240,000 (170,000 to 400,000), respectively [4]. Interestingly, the prevalence of people with HIV/AIDS accessing anti-retroviral therapy across sub-Sahara Africa ranges from 59.2% to 72.5% while that of Northern Africa was 38.3%. As of 2019, women and girls accounted for approximately 59% of those that were living with HIV in sub-Saharan Africa [4]. In sub-Saharan Africa, the prevalence of people living with HIV aged 15-49 years increased by 18.2% between 2000 and 2017 [5]. HIV facilitates HPV acquisition and delays its clearance with a concomitant increased risk of invasive cervical cancer (ICC) [6-9]. Belglaiaa et al. [10] maintained that HIV status is a strong predictor of high-risk HPV (hrHPV; odds ratio [OR], 4.16). Among HIV seropositive (HIV+) women, those who are positive for HIV-1/2 are 52% and 90% more like to be positive for hrHPVs than HIV-1+ and HIV-2+ women [11]. This suggests that the prevalence of HIV, especially HIV-1/2, may be responsible for the variation in the ASIR of cervical cancer between the African sub-regions. Additionally, a longer duration of HIV infection, higher viral load, and lower CD4 T-cell counts < 200/mm3 have also been implicated in a higher acquisition of HPV infection [12,13]. Considering race, in the United States, the incidence of HIV+ women diagnosed with cervical intraepithelial neoplasia grade 3 or higher was higher in African-Americans than Caucasians, with a ratio of 5:1. In the United States, the prevalent strains of hrHPV among HIV+ African-American women diagnosed with cervical cancer were HPV-16 (26.8%), HPV-53 (20.5%), HPV-35 (15.2%) and HPV-52/58 (14.3%) [14]. There is a paucity of data on the relationship between the types of HPV observed in African-American women and African women.
- The introduction of national HPV immunization programs in countries in sub-Saharan Africa started in 2011 [2]. As of 2019, only 17 countries out of the 46 countries (37.0%) in sub-Saharan Africa had established nationwide HPV immunization [15]. Studies show that the HPV vaccine coverage is higher in Northern Africa (35.6%) than in sub-Saharan Africa (1.2%) [15,16]. The difference in vaccine coverage between the 2 regions may account for the higher ASIR of cervical cancer in the latter than the former. The prevalence of HPV infection could serve as an alternative index for assessing the impact of HPV vaccination on the risk of developing cancer. Widely distributed HPV vaccines targeted at reducing cervical cancer include bivalent (HPV-16/18) and quadrivalent (HPV6/11/16/18). The third, nonavalent vaccine (Gardasil 9; 6/11/16/18/31/33/45/52/58), has yet to be widely distributed in most African countries [17]. Sexually transmitted HPV genotypes are grouped into the high-risk type (HPV-16, -18, -31, -33, -35, -39, -45, -51, -52, -56, -58, -59, -66, and -68) and low-risk type (HPV-6, -11, -26, -40, -73, and -82) based on epidemiologic association and potential risk of cervical cancer [18-21]. Of note, individuals infected with multiple hrHPV genotypes are more likely to develop large tumors and have a poor treatment response [22], owing to a high propensity of co-existing with other hrHPVs than low-risk HPVs [23]. The co-existence of the non-vaccine hrHPV reduces the efficacy of vaccines in preventing cervical cancer. According to Yar et al. [23], the involvement of non-vaccine hrHPV in hrHPV co-infections among African women was higher for HPV-35 (19.6%), followed by HPV-53 (15.0%), HPV-56 (7.5%), HPV-59/66 (6.5%), and HPV-82 (5.6%). Since the introduction of HPV vaccination into the national immunization program, to the best of our knowledge, no study has assessed the prevalence of HPV types, especially among HIV+ and HIV seronegative (HIV-) women, in sub-Saharan Africa between years up to 2010 and in 2011 and later; hence, the present review was conducted to address this gap in the research. This review suggests that a high prevalence of non-vaccine hrHPV and multiple HPV infections could be associated with the high ASIR of cervical cancer in sub-Saharan Africa.
INTRODUCTION
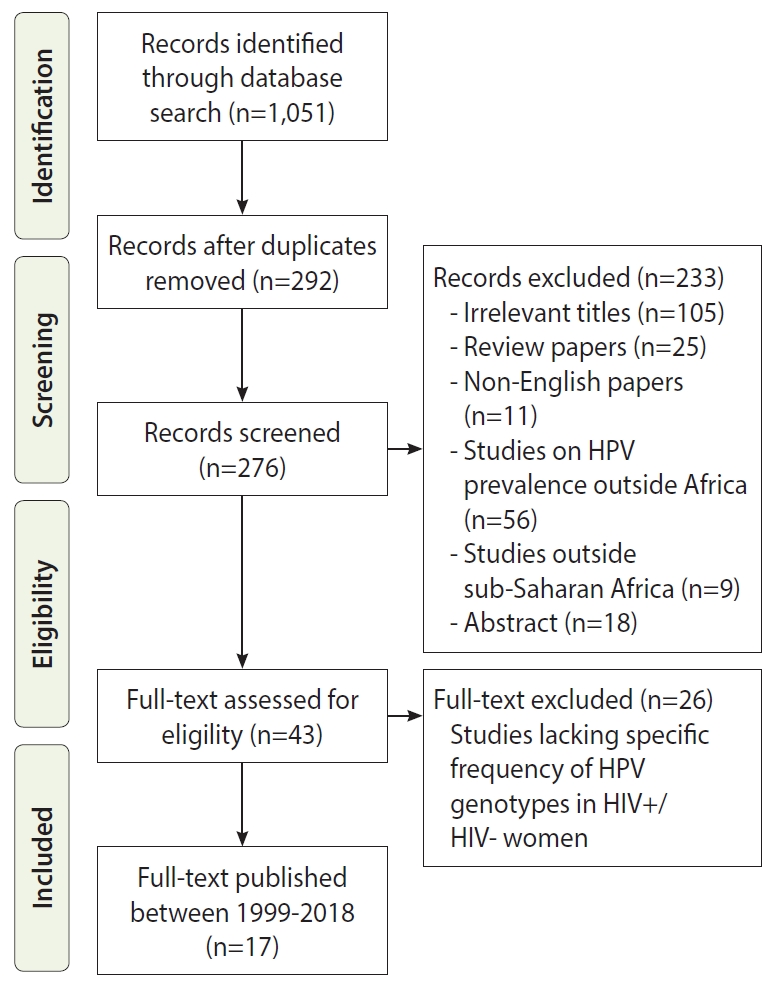
- This systematic review was carried out (up to September 16, 2020) in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines [24,25].
- Search strategy
- Studies that investigated the relationship between HIV status and HPV infection or acquisition were searched for in Google Scholar, Scopus, PubMed Central, and Embase databases and selected using the PRISMA guidelines (Figure 1). We screened the titles of cohort and case-controlled studies published between 1999 and 2018 using the following keywords and Medical Subject Headings (MeSH) terms: (‘HPV’ and ‘human papillomavirus’) AND (‘HIV’ and ‘human immunodeficiency virus’) AND (‘ICC’ and ‘invasive cervical cancer’) AND (‘prevalence’ OR ‘incidence’ OR ‘distribution’ OR ‘genotype’), AND (‘sub-Saharan Africa’). We also searched for unpublished studies (gray literature) by evaluating ClinicalTrials.gov (National Institutes of Health, NIH) and the International Clinical Trial Registry Platform (World Health Organization, WHO).
- Study quality assessment and study selection
- The quality of the included studies was assessed using an adapted version of the NIH’s Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies [26]. Three authors assessed the risk of bias (as good, unclear, or poor) in non-randomized observational studies across 5 criteria: study population, imprecision, inconsistency, bias in study design, and disclosure of conflict of interest [27,28]. The exclusion criteria were articles not written in English, abstracts, non-full-length articles, articles without specific frequency of HPV types, articles not involving Africa, and articles not dealing with cervical cancer. The inclusion criteria were studies that tested for hrHPV DNA, studies with specific frequency of hrHPV infection, and full-length articles involving sub-Saharan Africa.
- Only studies that used polymerase chain reaction, which is the gold standard for HPV testing, were included in this study (Tables 1-3). The overall prevalence of an HPV type (for example HPV-16) was dependent on the study size of studies that tested participants for the specific virus. In Figure 2A and B, the study of Menon et al. [19], which was carried out between 2009 and 2015, was excluded because its data cut across the 2 time periods (up to 2010 and in 2011 and later). The studies carried out by Diop-Ndiaye et al. [29], Dols et al. [30] and Denny et al. [31] were excluded from the calculations of the prevalence of multiple HPV infections due to lack of data (Table 4). The mean age of HIV+ and HIV- women did not include data from Mpunga et al. [32], Mudini et al. [20], Marembo et al. [33], Maranga et al. [34], and Banura et al. [35] because they did not specify the mean age and age range of the 2 groups. The data presented in Table 5 were only extracted from the studies carried out by Mpunga et al. [32], Mudini et al. [20], and Maranga et al. [34] due to the fact that their papers reported the prevalence of HPV types for both HIV+ and HIV- women diagnosed with cancer.
- Data extraction
- The essential information extracted for analysis included participant characteristics such as sample size, cases of HIV+ and HIV- women, the prevalence of any HPV infection and multiple HPV infections, HPV types (16, 18, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68, and 82), mean age, recruitment method, period of data collection, and study location and region (according to the WHO classification). We investigated the frequency of HPV infections in women living with HIV using HIV- women as the comparison group. When calculating the prevalence of any HPV infection (women who tested positive for any HPV type), an individual may have acquired multiple types (e.g., HPV-35 and -45) but it would only count as 1 event. The range of high-risk HPVs investigated in the selected studies varied; thus when calculating the prevalence of an HPV type, only studies or cases that investigated that particular HPV type were considered. To assess the impact of the time period on the prevalence of HPV infection, data points were categorized into a group until 2010 (inclusive) and a post-2010 group.
- Statistical analysis
- The ORs between HIV+ and HIV- women were also calculated in order to determine the risk of HPV acquisition and development of cervical cancer. Chi-square analysis was used to calculate the difference in HPV infection between HIV+ and HIV- women in Africa (GraphPad Prism version 6.0; GraphPad, San Diego, CA, USA), and the level of statistical significance was set at p-value ≤ 0.05.
- Ethics statement
- This review is exempt from ethical review and approval, since the secondary data used for pooled analysis were extracted from journal-related publications.
MATERIALS AND METHODS
- Selected studies and sample size
- Based on the inclusion criteria, 11 cross-sectional studies and 6 cohort studies were analyzed. Overall, this review included 16,237 participants (N) from 17 full-length articles (Figure 1 and Table 1). The number of HIV+ and HIV- women were 5,341 and 10,896, respectively. Southern Africa had the highest number of participants (10,285; n=3 studies), followed by West Africa (3,553; n=9 studies), and East Africa (2,399; n=5 studies), and Southern Africa (10,285; n=3 studies). The mean age of HIV- women was insignificantly higher than that of HIV+ women (38.1 vs. 36.2 years, p=0.59). The prevalence of HPV infection and multiple hrHPV infections in the cohort studies (which involved HIV+ women only) were twice the prevalence in the cross-sectional studies (which included both HIV+ and HIV- women). No cohort studies involving only HIV- women were identified. The 3 most prevalent HPV types in the cohort studies were HPV-52, HPV-16, and HPV-35, while those in the cross-sectional studies were HPV-16, HPV-18, and HPV-35 (Table 2). Table 3 shows the summary of the findings from each study.
- Prevalence of human papillomavirus (HPV) and multiple HPV infections in the general population
- The prevalence of various HPV types and multiple HPV infections was higher in HIV+ women than in HIV-women (p<0.001) (Table 4). The most prevalent HPV type in the general population of sub-Saharan Africa was HPV-16, followed in order by HPV-66, HPV-53, and HPV-52. Furthermore, HIV+ women in subSahara Africa were approximately 3 times and 4 times more likely to be HPV-infected and to have multiple HPV infections, respectively (Table 4). Table 4 also shows that HIV+ women were approximately 2 times, 3 times, 4 times, and 5 times more likely to acquire HPV-16/-18/-33/-45/-53/-59, HPV-31/-35/-56/-58/-68, HPV-39/-52, and HPV-82, respectively than their HIV- counterparts. HIV+ women were 26% more likely to acquire HPV-66 than HIV- women.
- Human papillomavirus infection and study timing
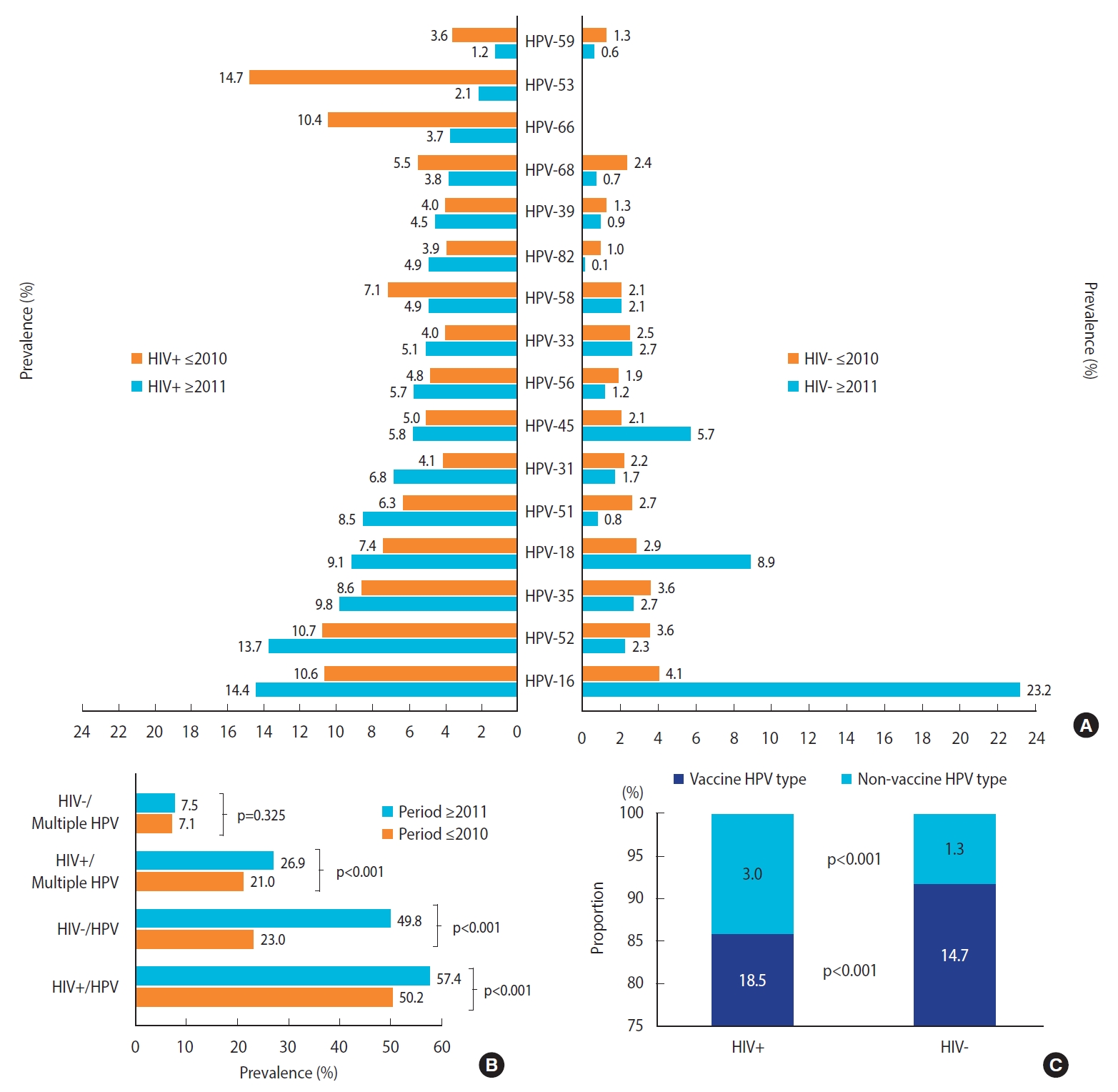
- Between 1999-2010 and 2011-2018, the prevalence of HPV-16, HPV-18, and HPV-45 among HIV- and HIV+ women increased by 19.1%p versus 3.8%p, 6.0%p versus 1.7%p, and 3.6%p versus 0.8%p, respectively (Figure 2). Furthermore, the prevalence of HPV-53, HPV-66, HPV-59, HPV-58, and HPV-68 decreased by 12.6%p, 6.7%p, 2.4%p, 2.2%p, and 1.7%p among HIV+ women, respectively. Overall, the prevalence of HPV and multiple HPV infections increased in sub-Sahara Africa within the study period (Figure 2).
- As shown in Figure 2A, in sub-Saharan Africa, the prevalence of HPV types among HIV- women up to 2010 was higher than in 2011 and later, except for HPV-16, HPV-18, and HPV-45. Furthermore, the prevalence of HPV types among HIV+ women up to 2010 was lower than in 2011 and later, except for HPV-58, HPV68, HPV-66, HPV-53, and HPV-59. A higher prevalence of HPV infection was observed in 2011 and later than up to 2010 both in HIV+ and HIV- women (Figure 2B). The difference in the prevalence of HPV infection, the difference between 2011 and later and up to 2010 was higher among HIV- women than in HIV+ women (26.8 vs. 7.2%). Among HIV- women, the prevalence of HPV infection doubled between 2010 and 2018, unlike HPV prevalence in HIV+ women, which increased by 5.4%p (Figure 2B). Furthermore, a higher prevalence of multiple HPV infections was observed in 2011 and later than up to 2010 both in HIV+ women (p<0.05) and HIV- women (p>0.05). In Figure 2C, a higher prevalence of vaccine and non-vaccine HPV types were observed among HIV+ women when compared with their HIV- counterparts (18.5 vs. 14.7%, and 3.0 vs. 1.3%, respectively at p<0.001). However, a higher frequency of vaccine HPV types was observed among HIV- women than among HIV+ women (91.9 vs. 86.0%), whereas a higher frequency of non-vaccine HPV types was observed among HIV+ women than among HIV- women (14.0 vs. 8.1%) at p<0.001.
- Prevalence of multiple infections and human papillomavirus types among women with cervical cancer
- Among women diagnosed with ICC, the prevalence of multiple HPV infections was higher in HIV+ women than in HIV- women (28.9 vs. 13.1%, respectively; p<0.001). In descending order, the most prevalent hrHPV types among HIV+ and HIV- women diagnosed with ICC were HPV-16 (51.9 vs. 58.2%), HPV-18 (24.6 vs. 18.5%), and HPV-45 (12.8 vs. 12.6%, respectively). Significant differences between HIV+ and HIV- women diagnosed with ICC were only observed for the prevalence of HPV-56 (7.3 vs. 1.3%), HPV-31 (5.3 vs. 2.2%), and HPV-51 (3.3 vs. 0.4%, respectively) at p<0.001, p=0.050, and p=0.013, respectively. HIV+ women in sub-Saharan Africa who were positive for HPV-56/51 and HPV-68 were 6 times and 5 times more likely to develop cervical cancer than their HIV- counterparts (p<0.001/p=0.013 and p=0.125, respectively). Figure 2 also shows that HIV+ women with multiple HPV infections and HPV-31/-39/-58 were approximately 3 times more likely to develop cervical cancer than HIV- women. Furthermore, HIV+ women with HPV-16 and HPV-35 were 23% and 51% less likely to develop cervical cancer than their HIV- counterparts (Table 5). As shown in Table 5, the prevalence of all HPV types, including multiple HPV types, was higher among HIV+ women than among HIV- women, except HPV-16 and HPV-35.
RESULTS
- This study assessed the prevalence of HPV types among HIV+ and HIV- women in regions of sub-Saharan Africa and between 2 time intervals: up to 2010 and 2011 and later. The prevalence of HPV and multiple HPV infections was higher among HIV+ women than among HIV- women living in sub-Saharan Africa. Between 2013 and 2016, this pattern of infection was also observed among HIV+ and HIV- women in North Africa (65.7 vs. 13.3% and 38.5 vs. 7.6% respectively) [10,13]. The lower ASIR of cervical cancer in North Africa could be attributed to higher HPV vaccine coverage than in sub-Saharan Africa [16]. Conversely, the reason(s) for the differences between HIV+ and HIV- women are not well-understood. However, previous studies [11,42] opined that HIV+ women initiate sex at a younger age, and therefore have a higher number of lifetime sexual partners, in turn increasing their risk of acquisition and persistence of HPV infections relative to their HIV- counterparts. As of 2016, the review carried out by Clifford et al. [8] shows that HPV-16 (46.6%), HPV-18 (24.4%), and HPV-45 (15.5%) were the prevalent HPV types in HIV+ women diagnosed with ICC in Africa. Our findings further show that HPV-16, HPV-18, and HPV-45 were the prevalent HPV types not only among HIV+ women, but also among HIV- women in sub-Saharan Africa. The prevalence of HPV-16 and HPV-18 among HIV+ women in this review were higher than that of Clifford et al. [8], possibly due to differences in study timelines and regions involved [11]. The differences observed between HIV+ and HIV- women suggest that the prevalence of HIV in a population increases the risk of acquiring HPV and multiple infections [20,29,34]. These factors, in turn, predict a disproportionate ASIR of cervical cancer among HIV+ and HIV- women in sub-regions of Africa [19]. Additionally, in sub-Saharan Africa, the prevalence of HPV-16 and HPV-35 infections was higher in HIV- women diagnosed with ICC than in their HIV+ counterparts. The reason for this is unknown.
- Studies have shown that HPV-infected women, especially those infected with hrHPV types, are approximately at a 2-fold higher risk of acquiring HIV than HPV-uninfected women [43,44]. A follow-up investigation carried out among HIV-uninfected women showed that 28.4% of HPV-infected women seroconverted after an average of 2.4 years. The study revealed that women with multiple hrHPV infections were 4 times more likely to acquire HIV than those with a single or no hrHPV infection [45]. The high-risk of developing cervical cancer among HIV+ women and the risk of seroconversion among HIV- women due to the high prevalence of multiple HPV infections may account for the high ASIR of cervical cancer in sub-Saharan Africa [1]. According to Smith-McCune et al. [46], women with nonavalent vaccine types are 2.5 times more likely to acquire HIV than women with vaccine HPV types. The high ASIR of cervical cancer in sub-Saharan Africa, when compared to North Africa may be due to a higher prevalence of nonavalent hrHPV among HIV+ and HIV- women. Of note, the most prevalent HPV types among HIV+ women in North Africa were vaccine HPV types: HPV-58 (22.1%), HPV-18 (7.8%), HPV-16 (7.3%), HPV-33 (6.0%), and HPV-52 (3.7%) [10,13]. Conversely, in order of prevalence, the most prevalent HPV types among people living with HIV in sub-Saharan Africa irrespective of cytology status were HPV-16, HPV-52, HPV-53, HPV-35, and HPV-66. This suggests that with the available vaccine, it could be easier to reduce or prevent cervical cancer attributable to HPV in North Africa than in sub-Saharan Africa. Taken together, HIV+ women in sub-Saharan Africa are at a higher risk of developing cervical cancer despite the available vaccine due to a higher prevalence of non-vaccine hrHPV types. Since women who are HPV-16 and HPV-18-positive are 11-22 times and 45-58 times capable of acquiring other hrHPV types, respectively [47], it could be argued that the lower prevalence of non-vaccine HPV types among HIV+ women in North Africa, when compared with their sub-Sahara African counterparts, was due to the low prevalence of HPV-16 and HPV-18 (Table 4).
- This study revealed that the prevalence of HPV-16, HPV-18, and HPV-45 increased from the time period up to 2010 to 2011 and later in both HIV+ and HIV- women. The increase could be due to increasing awareness of cervical cancer and uptake of screening services, better screening and testing techniques or protocols, or changes in policy. Interestingly, the percentage difference in HPV infection between up to 2010 and 2011 and later was considerably higher in HIV- women. The reason for this is also unknown. Similarly, the changes in the prevalence of HPV-16 between both time periods among HIV+ and HIV- women were significant (p<0.001), but substantially higher among HIV-women than in HIV+ women (Figure 1). This agrees with the findings of Dames et al. [12] showing lower HPV infection among women with CD4+ T-cell counts of ≥ 200 cells/mm3. On the other hand, increased sexual behavior or activity and a higher frequency of unprotected sex may be responsible for the marked increase in HPV prevalence among HIV- women in sub-Saharan Africa. Low CD4+ T-cell counts, lower age, a history of multiple sexual partners, and a high number of unprotected sexual intercourse, especially among infected persons living with HIV [13,31] may also be responsible for multiple HPV infections among HIV+ women.
- Based on the database search, studies from Central Africa did not meet the inclusion criteria. Since Central Africa is a sub-region of sub-Saharan Africa, the non-inclusion of studies from the sub-region constitutes a limitation of this study. Moreover, in this study, a meta-analysis was not carried out; hence, there could be possibility of some publication bias or heterogeneity.
DISCUSSION
- This paper reveals that the prevalence of HPV infection, multiple HPV infections, and non-vaccine HPV types were higher among HIV+ women than in HIV- women in sub-Saharan Africa. This paper revealed that the prevalence of hrHPV, especially HPV-16 and HPV-18, increased over the last decade irrespective of HIV status. Although HIV infection influences the distribution of HPV types, this study suggests that cervical cancer incidence in sub-Saharan Africa is primarily driven by the prevalence of vaccine hrHPVs, especially HPV-16 and HPV-18.
CONCLUSION
-
CONFLICT OF INTEREST
The authors have no conflicts of interest to declare for this study.
-
FUNDING
None.
-
AUTHOR CONTRIBUTIONS
Conceptualization: JOO. Data curation: JOO, OKA. Formal analysis: JOO, CAO. Funding acquisition: None. Methodology: JOO, OKA, OO. Visualization: OO, CAO. Writing – original draft: JOO, OO. Writing – review & editing: JOO, CAO, OKA, OO.
NOTES
ACKNOWLEDGEMENTS

| Study | Location | Period of study | Mean age (range), yr | Study size | Multiple HPV (%) | Order of 6 most prevalent high-risk HPV types | |
|---|---|---|---|---|---|---|---|
| Studies of HIV seropositive women | |||||||
| Mpunga et al. [32]1 | Rwanda | 2012-2018 | 54.3 (NA)4 | 99 | 7 (7.2) | 16, 35, 45, 31, 33, 52 | |
| Yakub et al. [18] | Nigeria | 2016-2017 | NA (20-50) | 220 | 25 (11.4) | 35, 16, 45, 33, 18, 56 | |
| Ndizeye et al. [36] | Burundi | 2013/2016 | 39.9 (NA) | 301 | 28 (9.3) | 16, 18, 51, 52, 58, 56/66 | |
| Mudini et al. [20]1 | Zimbabwe | 2014-2015 | NA (40-60)4 | 53 | 30 (56.6) | 16, 18, 56, 45, 33, 58 | |
| Obiri-Yeboah et al. [37] | Ghana | 2017 | 43.8 (NA) | 160 | 77 (48.1) | 35, 52, 58, 16, 18, 68 | |
| Marembo et al. [33] | Zimbabwe | 2015 | 39.8 (18-83)4 | 70 | 17 (24.3) | 52, 16, 18, 58, 51, 31/33/45 | |
| Menon et al. [19]2 | Kenya | 2009-2015 | 28.0 (NA) | 74 | 48 (64.9) | 16, 53, 52, 56, 18/35/58, | |
| Ezechi et al. [38] | Nigeria | 2014 | NA (NA) | 220 | 18 (8.2) | 16, 35, 31, 58, 52, 18/45 | |
| Akarolo-Anthony et al. [21] | Nigeria | 2012 | 36.6 (NA) | 149 | 21 (14.1) | 35, 56, 58, 59, 45, 33 | |
| Kelly et al. [39] | SA | 2011-2012 | NA (20-50) | 594 | 147 (24.7) | 52, 51, 35, 16, 31, 39 | |
| Kelly et al. [39] | Burkina Faso | 2011-2012 | NA (20-50) | 621 | 271 (43.6) | 52, 16, 35, 51, 18, 31 | |
| Diop-Ndiaye et al. [29]3 | Senegal | 2010 | 36.0 (30-45) | 67 | NA | 52, 16, 68, 35, 45, 51 | |
| Dols et al. [30] | Tanzania/SA | 2008-2010 | NA (NA) | 194 | NA | 52, 16, 51, 35, 58, 18 | |
| Guthrie et al. [40] | Kenya | 2007-2009 | NA (18-50) | 283 | 122 (43.1) | 52, 18, 16, 51, 35, 68 | |
| Maranga et al. [34] | Kenya | 2008-2009 | 35.3 (21-50)4 | 113 | 22 (19.5) | 52, 56, 58, 53, 16, 35/39/66 | |
| McDonald et al. [41] | SA | 1999-2006 | NA (26-38) | 1641 | 249 (15.2) | 35, 16, 58, 18, 68, 45 | |
| Banura et al. [35] | Uganda | 2002-2004 | NA (12-24)4 | 82 | 53 (64.6) | 52, 33, 16, 51, 68, 66 | |
| Denny et al. [31] | SA | 2000-2003 | 29.3 (18-54) | 400 | NA | 16, 52, 53, 35, 18, 58 | |
| Studies of HIV seronegative women | |||||||
| Mpunga et al. [32]1 | Rwanda | 2012-2018 | 54.3 (NA)4 | 501 | 21 (4.2) | 16, 18, 45, 33, 35, 52 | |
| Ndizeye et al. [36] | Burundi | 2013/2016 | 36.4 (NA) | 299 | 9 (3.0) | 16, 18, 66, 45, 58, 53 | |
| Mudini et al. [20]1 | Zimbabwe | 2014-2015 | NA (40-60)4 | 54 | 25 (46.3) | 16, 13, 33, 35, 56, 45 | |
| Obiri-Yeboah et al. [37] | Ghana | 2017 | 44.3 (NA) | 169 | 36 (21.3) | 35, 33, 58, 56, 52, 18/39/68 | |
| Marembo et al. [33] | Zimbabwe | 2015 | 39.8 (18-83)4 | 66 | 10 (15.2) | 18, 16, 52, 31, 45/51/58 | |
| Ezechi et al. [38] | Nigeria | 2014 | NA (NA) | 295 | 10 (3.4) | 18, 58, 16, 52, 31/35/51 | |
| Akarolo-Anthony et al. [21] | Nigeria | 2012 | 37.6 (NA) | 108 | 2 (1.9) | 52, 68, 18, 39, 45, 16/31/56/59 | |
| Diop-Ndiaye et al. [29]2 | Senegal | 2010 | 34.0 (26-42) | 369 | NA | 52, 64, 16, 51, 35, 31/33 | |
| Maranga et al. [34] | Kenya | 2008-2009 | 35.3 (21-50)4 | 111 | 15 (13.5) | 56, 16, 33, 35, 59, 51/52/82 | |
| McDonald et al. [41] | SA | 1999-2006 | NA (33-45) | 8,050 | 301 (3.7) | 35, 16, 58, 45, 52, 18 | |
| Banura et al. [35] | Uganda | 2002-2004 | NA (12-24)4 | 868 | 324 (37.3) | 18, 52, 16, 51, 33, 68 | |
| Study | Countries | Study period | Cases, n | High-risk HPV (%) | Multiple-HPV prevalence (%) | Order of 6 most prevalent high-risk HPV types | |
|---|---|---|---|---|---|---|---|
| Cross-sectional studies (HIV+/HIV-) | |||||||
| Mpunga et al. [32]1 | Rwanda | 2012-2018 | 598 | 574 (96.0) | 28 (4.7) | 16, 18, 45, 33, 35, 52 | |
| Mudini et al. [20]1 | Zimbabwe | 2014-2015 | 107 | 101 (94.4) | 55 (51.4) | 16, 18, 56, 33, 45, 35 | |
| Banura et al. [35] | Uganda | 2002-2004 | 950 | 707 (74.4) | 377 (39.7) | 52,16, 18, 51, 33, 56 | |
| Diop-Ndiaye et al. [29]2 | Senegal | 2010 | 436 | 316 (72.5) | NA | 52, 16, 68, 35, 51, 33 | |
| Marembo et al. [33] | Zimbabwe | 2015 | 136 | 70 (51.5) | 27 (19.9) | 18, 52, 16, 58, 51, 31 | |
| Obiri-Yeboah et al. [37] | Ghana | 2017 | 329 | 156 (47.4) | 113 (34.3) | 35, 58, 52, 18, 56, 16/56 | |
| Maranga et al. [34] | Kenya | 2008-2009 | 224 | 105 (46.9) | 37 (16.5) | 56, 52, 58, 16, 35, 33 | |
| Akarolo-Anthony et al. [21] | Nigeria | 2012 | 257 | 64 (24.9) | 23 (8.9) | 82, 35, 56, 58, 45, 59 | |
| Ndizeye et al. [36] | Burundi | 2013/2016 | 600 | 142 (23.7) | 37 (6.2) | 16, 18, 58, 52, 51, 31 | |
| Ezechi et al. [38] | Nigeria | 2014 | 515 | 101 (19.6) | 28 (5.4) | 16, 35, 58, 31, 18, 52 | |
| McDonald et al. [41] | SA | 1999-2006 | 9,691 | 1,848 (19.1) | 550 (5.7) | 35, 16, 58, 45, 18, 52 | |
| Total [20, 21, 29, 32-38, 41] | Africa | 1999-2018 | 13,843 | 4,184 (30.2) | 1,275 (9.5) | 16, 18, 35, 52, 45, 58 | |
| Cohort studies (HIV+ only) | |||||||
| Yakub et al. [18] | Nigeria | 2016-2017 | 220 | 83 (37.7) | 25 (11.4) | 35, 16, 45, 33, 18, 56 | |
| Menon et al. [19]3 | Kenya | 2009-2015 | 74 | 52 (70.2) | 48 (64.9) | 16, 53, 52, 56, 18/35/58 | |
| Kelly et al. [39] | Burkina Faso | 2011-2012 | 621 | 491 (79.1) | 271 (43.6) | 52, 16, 35, 51, 18, 31 | |
| Kelly et al. [39] | SA | 2011-2012 | 594 | 351 (59.1) | 147 (24.7) | 52, 51, 35, 16, 31, 39 | |
| Dols et al. [30] | Tanzania/SA | 2008-2010 | 194 | 109 (56.2) | NA | 52, 16, 51, 35, 58, 18 | |
| Guthrie et al. [40] | Kenya | 2007-2009 | 283 | 176 (62.2) | 122 (43.1) | 52, 18, 16, 51, 35, 68 | |
| Denny et al. [31] | SA | 2000-2003 | 400 | 301 (75.3) | NA | 16, 52, 53, 35, 18, 58 | |
| Total [18, 19, 30, 31, 39, 40] | Africa | 2000-2017 | 2,386 | 1,563 (65.5) | 613 (34.2) | 52, 16, 35, 18, 51, 31 | |
| Study | Location | Summary/Inferences |
|---|---|---|
| Mpunga et al. [32]1 | Rwanda | There was a minimal impact of HIV on HPV type distribution |
| Yakub et al. [18] | Nigeria | HIV+ women with a low CD4+ T count were at a higher risk of cervical precancerous lesions |
| Ndizeye et al. [36] | Burundi | There was a high burden of hrHPV and phrHPV infections among women with HIV; The nonavalent vaccine covered most of the hrHPV infections irrespective of residential area and HIV status |
| Mudini et al. [20]1 | Zimbabwe | HIV may influence the distribution of some HPV genotypes given the significant increase in prevalence of HPV-18 among HIV+ women; The proportion of women with multiple genotypes was high and almost equal in both HIV+ and HIV- women |
| Obiri-Yeboah et al. [37] | Ghana | HIV-1 infected women bore a significant burden of HPV infection and related disease; The nonavalent HPV vaccine is likely the best means of cervical cancer prevention in Ghana |
| Marembo et al. [33] | Zimbabwe | There was an increased risk of hrHPV infection as well as multiple hrHPV genotypes in HIV+ women |
| Menon et al. [19]2 | Kenya | Co-infection with phrHPV and hrHPV genotypes was more strongly associated with abnormal cytology than any single hrHPV; There was a high prevalence of multiple hrHPV genotypes in FSW, especially in HIV+ women |
| Ezechi et al. [38] | Nigeria | HPV-16, -35, -58, and -31 were the most common hrHPV infections in the population and HIV+ women awere at higher risk of acquiring HPV infection; Current HPV vaccines prevented genotypes 16 and 18, which accounted for only a minority of hrHPV infection (21.7%) with no significant difference been HIV+ and HIV- women |
| Akarolo-Anthony et al. [21] | Nigeria | There was a high prevalence of non-16 and -18 hrHPV among HIV+ women in Nigeria and other African countries |
| Kelly et al. [39] | SA/Burkina Faso | hrHPV infections and cervical lesions were very common among HIV+ women in Africa; Bivalent or quadrivalent vaccines could prevent up to 45% of treatable precursor lesions, and the nonavalent vaccine could prevent up to 90% of cases in HIV+ women |
| Diop-Ndiaye et al. [29]3 | Senegal | HPV-16 and -35 were the most prevalent HPV types among HIV-infected FSW |
| Dols et al. [30] | Tanzania/SA | More than one-third (42%) of women with normal cytology tested positive for hrHPV |
| Guthrie et al. [40] | Kenya | hrHPV prevalence was high in HIV+ women; Screening for hrHPV genotypes would identify a large majority of women who have high-grade cervical lesions or more severe cytology |
| Maranga et al. [34] | Kenya | HIV infection appeared to alter the spectrum of HPV types found in both cervical smears and invasive cervical carcinomas; HPV infections were associated with a reduced level of immunity |
| McDonald et al. [41] | SA | HPV-16 and -35 were the prevalent HPV types among HIV+ and HIV- women with or without cervical disease |
| Banura et al. [35] | Uganda | There was an elevated prevalence of HPV infection in HIV+ and HIV- young women |
| Denny et al. [31] | SA | There was a high level of hrHPV infections in HIV-1 infected women |
HIV, human immunodeficiency virus; HPV, human papillomavirus; hrHPV, high-risk human papillomavirus; phrHPV, probable high-risk human papillomavirus; HIV+, human immunodeficiency virus seropositive; HIV-, human immunodeficiency virus seronegative; SA, South Africa; FSW, female sex workers.
1 Cancer.
2 FSW with abnormal cytology.
3 FSW.
| HPV type |
HIV seropositive |
HIV seronegative |
% Diff (n1-n2) | Rank | OR (95% CI) | p-value1 | ||
|---|---|---|---|---|---|---|---|---|
| Cases, N | HPV, n1 (%) | Cases, N | HPV, n2 (%) | |||||
| Multiple | 187 | 54 (28.9) | 595 | 78 (13.1) | 15.8 | - | 2.69 (1.81, 4.00) | <0.001 |
| HPV-16 | 187 | 97 (51.9) | 595 | 346 (58.2) | -6.3 | 1 | 0.77 (0.56, 1.08) | 0.150 |
| HPV-18 | 187 | 46 (24.6) | 595 | 110 (18.5) | 6.1 | 2 | 1.43 (0.97, 2.12) | 0.075 |
| HPV-45 | 187 | 24 (12.8) | 595 | 75 (12.6) | 0.2 | 14 | 1.02 (0.62, 1.67) | 0.900 |
| HPV-56 | 150 | 11 (7.3) | 555 | 7 (1.3) | 6.0 | 3 | 6.18 (0.85, 2.79) | <0.001 |
| HPV-33 | 150 | 9 (6.0) | 555 | 31 (5.6) | 0.4 | 13 | 1.08 (0.51, 2.32) | 0.843 |
| HPV-31 | 150 | 8 (5.3) | 555 | 12 (2.2) | 3.1 | 4 | 2.55 (1.02, 6.35) | 0.050 |
| HPV-58 | 150 | 7 (4.7) | 555 | 9 (1.6) | 3.1 | 4 | 2.96 (1.08, 8.08) | 0.060 |
| HPV-66 | 53 | 2 (3.7) | 54 | 1 (1.9) | 1.8 | 7 | 2.08 (0.70, 23.57) | 0.618 |
| HPV-82 | 53 | 2 (3.7) | 54 | 1 (1.9) | 1.8 | 7 | 2.08 (0.70, 23.57) | 0.618 |
| HPV-51 | 150 | 5 (3.3) | 555 | 3 (0.4) | 2.9 | 6 | 6.34 (1.52, 26.58) | 0.013 |
| HPV-52 | 150 | 4 (2.7) | 555 | 14 (2.5) | 0.2 | 14 | 1.06 (0.34, 3.29) | 1.000 |
| HPV-68 | 97 | 2 (2.1) | 501 | 2 (0.4) | 1.7 | 9 | 5.25 (0.73, 37.7) | 0.125 |
| HPV-35 | 150 | 3 (2.0) | 555 | 22 (4.0) | 1.6 | 10 | 0.49 (0.15, 1.67) | 0.325 |
| HPV-39 | 150 | 3 (2.0) | 555 | 4 (0.7) | 1.3 | 11 | 2.81 (0.61, 12.7) | 0.170 |
| HPV-59 | 150 | 2 (1.3) | 555 | 3 (0.5) | 0.8 | 12 | 2.49 (0.41, 15.0) | 0.289 |
| HPV-53 | 37 | 0 (0.0) | 40 | 0 (0.0) | 0.0 | 16 | - | - |
- 1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018;68:394-424.ArticlePubMed
- 2. Black E, Richmond R. Prevention of cervical cancer in sub-Saharan Africa: the advantages and challenges of HPV vaccination. Vaccines (Basel) 2018;6:61.ArticlePubMedPMC
- 3. Jedy-Agba E, Joko WY, Liu B, Buziba NG, Borok M, Korir A, et al. Trends in cervical cancer incidence in sub-Saharan Africa. Br J Cancer 2020;123:148-154.ArticlePubMedPMC
- 4. United Nations Programme on HIV/AIDS (UNAIDS). Fact sheet 2021: preliminary UNAIDS 2021 epidemiological estimates. [cited 2020 Nov 28]. Available from: https://www.unaids.org/sites/default/files/media_asset/UNAIDS_FactSheet_en.pdf.
- 5. Dwyer-Lindgren L, Cork MA, Sligar A, Steuben KM, Wilson KF, Provost NR, et al. Mapping HIV prevalence in sub-Saharan Africa between 2000 and 2017. Nature 2019;570:189-193.ArticlePubMedPMC
- 6. Massad LS, Xie X, Burk R, Keller MJ, Minkoff H, DʼSouza G, et al. Long-term cumulative detection of human papillomavirus among HIV seropositive women. AIDS 2014;28:2601-2608.ArticlePubMed
- 7. Rowhani-Rahbar A, Hawes SE, Sow PS, Toure P, Feng Q, Dem A, et al. The impact of HIV status and type on the clearance of human papillomavirus infection among Senegalese women. J Infect Dis 2007;196:887-894.ArticlePubMed
- 8. Clifford GM, Tully S, Franceschi S. Carcinogenicity of human papillomavirus (HPV) types in HIV-positive women: a meta-analysis from HPV infection to cervical cancer. Clin Infect Dis 2017;64:1228-1235.ArticlePubMedPMC
- 9. Abraham AG, Strickler HD, D’Souza G. Invasive cervical cancer risk among HIV-infected women is a function of CD4 count and screening. J Acquir Immune Defic Syndr 2013;63:e163.ArticlePMC
- 10. Belglaiaa E, Elannaz H, Mouaouya B, Aksim M, Mercier M, Prétet JL, et al. Human papillomavirus genotypes among women with or without HIV infection: an epidemiological study of Moroccan women from the Souss area. Infect Agent Cancer 2015;10:44.ArticlePubMedPMC
- 11. Hanisch RA, Sow PS, Toure M, Dem A, Dembele B, Toure P, et al. Influence of HIV-1 and/or HIV-2 infection and CD4 count on cervical HPV DNA detection in women from Senegal, West Africa. J Clin Virol 2013;58:696-702.ArticlePubMedPMC
- 12. Dames DN, Blackman E, Butler R, Taioli E, Eckstein S, Devarajan K, et al. High-risk cervical human papillomavirus infections among human immunodeficiency virus-positive women in the Bahamas. PLoS One 2014;9:e85429.ArticlePubMedPMC
- 13. Ouladlahsen A, Fayssel N, Bensghir R, Baba H, Lamdini H, Sodqi M, et al. The human papillomavirus among women living with human immunodeficiency virus in Morocco: a prospective crosssectional study. J Infect Dev Ctries 2018;12:477-484.ArticlePubMed
- 14. Keller MJ, Burk RD, Massad LS, Eltoum IE, Hessol NA, Anastos K, et al. Racial differences in HPV types amongst US women with HIV and cervical precancer. AIDS 2018;32:2821-2826.ArticlePubMed
- 15. Amponsah-Dacosta E, Kagina BM, Olivier J. Health systems constraints and facilitators of human papillomavirus immunization programmes in sub-Saharan Africa: a systematic review. Health Policy Plan 2020;35:701-717.ArticlePubMedPMC
- 16. Klein C, Kahesa C, Mwaiselage J, West JT, Wood C, Angeletti PC. How the cervical microbiota contributes to cervical cancer risk in sub-Saharan Africa. Front Cell Infect Microbiol 2020;10:23.ArticlePubMedPMC
- 17. Meites E, Szilagyi PG, Chesson HW, Unger ER, Romero JR, Markowitz LE. Human papillomavirus vaccination for adults: updated recommendations of the Advisory Committee on Immunization Practices. MMWR Morb Mortal Wkly Rep 2019;68:698-702.ArticlePubMedPMC
- 18. Yakub MM, Fowotade A, Anaedobe CG, Manga MM, Bakare RA, Abimiku BA. Human papillomavirus correlates of high grade cervical dysplasia among HIV-Infected women at a major treatment centre in Nigeria: a cross-sectional study. Pan Afr Med J 2019;33:125.ArticlePubMedPMC
- 19. Menon SS, Rossi R, Harebottle R, Mabeya H, Vanden Broeck D. Distribution of human papillomaviruses and bacterial vaginosis in HIV positive women with abnormal cytology in Mombasa, Kenya. Infect Agent Cancer 2016;11:17.ArticlePubMedPMC
- 20. Mudini W, Palefsky JM, Hale MJ, Chirenje MZ, Makunike-Mutasa R, Mutisi F, et al. Human papillomavirus genotypes in invasive cervical carcinoma in HIV-seropositive and HIV-seronegative women in Zimbabwe. J Acquir Immune Defic Syndr 2018;79:e1-e6.ArticlePubMedPMC
- 21. Akarolo-Anthony SN, Famooto AO, Dareng EO, Olaniyan OB, Offiong R, Wheeler CM, et al. Age-specific prevalence of human papilloma virus infection among Nigerian women. BMC Public Health 2014;14:656.ArticlePubMedPMC
- 22. Bello BD, Spinillo A, Alberizzi P, Cesari S, Gardella B, D’Ambrosio G, et al. Cervical infections by multiple human papillomavirus (HPV) genotypes: prevalence and impact on the risk of precancerous epithelial lesions. J Med Virol 2009;81:703-712.ArticlePubMed
- 23. Yar DD, Salifu SP, Darko SN, Annan AA, Gyimah AA, Buabeng KO, et al. Genotypic characterisation of human papillomavirus infections among persons living with HIV infection; a case-control study in Kumasi, Ghana. Trop Med Int Health 2016;21:275-282.ArticlePubMed
- 24. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med 2009;6:e1000100.ArticlePubMedPMC
- 25. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 2009;6:e1000097.ArticlePubMedPMC
- 26. National Heart, Lung, and Blood Institute. Assessing cardiovascular risk: systematic evidence review from the Risk Assessment Work Group; 2013 [cited 2020 Mar 2]. Available from: https://www.nhlbi.nih.gov/health-topics/assessing-cardiovascular-risk.
- 27. Sanderson S, Tatt ID, Higgins JP. Tools for assessing quality and susceptibility to bias in observational studies in epidemiology: a systematic review and annotated bibliography. Int J Epidemiol 2007;36:666-676.ArticlePubMed
- 28. Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016;355:i4919.ArticlePubMedPMC
- 29. Diop-Ndiaye H, Beiter K, Gheit T, Sow Ndoye A, Dramé A, McKay-Chopin S, et al. Human papillomavirus infection in Senegalese female sex workers. Papillomavirus Res 2019;7:97-101.ArticlePubMedPMC
- 30. Dols JA, Reid G, Brown JM, Tempelman H, Bontekoe T, Quint WG, et al. HPV type distribution and cervical cytology among HIV-positive Tanzanian and South African women. ISRN Obstet Gynecol 2012;2012:514146.ArticlePubMedPMC
- 31. Denny L, Boa R, Williamson AL, Allan B, Hardie D, Stan R, et al. Human papillomavirus infection and cervical disease in human immunodeficiency virus-1-infected women. Obstet Gynecol 2008;111:1380-1387.ArticlePubMed
- 32. Mpunga T, Chantal Umulisa M, Tenet V, Rugwizangoga B, Milner DA Jr, Munyanshongore C, et al. Human papillomavirus genotypes in cervical and other HPV-related anogenital cancer in Rwanda, according to HIV status. Int J Cancer 2020;146:1514-1522.ArticlePubMed
- 33. Marembo T, Dube Mandishora R, Borok M. Use of multiplex polymerase chain reaction for detection of high-risk human papillomavirus genotypes in women attending routine cervical cancer screening in Harare. Intervirology 2019;62:90-95.ArticlePubMed
- 34. Maranga IO, Hampson L, Oliver AW, He X, Gichangi P, Rana F, et al. HIV Infection alters the spectrum of HPV subtypes found in cervical smears and carcinomas from Kenyan women. Open Virol J 2013;7:19-27.ArticlePubMedPMC
- 35. Banura C, Franceschi S, Doorn LJ, Arslan A, Wabwire-Mangen F, Mbidde EK, et al. Infection with human papillomavirus and HIV among young women in Kampala, Uganda. J Infect Dis 2008;197:555-562.ArticlePubMed
- 36. Ndizeye Z, Vanden Broeck D, Lebelo RL, Bogers J, Benoy I, Van Geertruyden JP. Prevalence and genotype-specific distribution of human papillomavirus in Burundi according to HIV status and urban or rural residence and its implications for control. PLoS One 2019;14:e0209303.ArticlePubMedPMC
- 37. Obiri-Yeboah D, Akakpo PK, Mutocheluh M, Adjei-Danso E, Allornuvor G, Amoako-Sakyi D, et al. Epidemiology of cervical human papillomavirus (HPV) infection and squamous intraepithelial lesions (SIL) among a cohort of HIV-infected and uninfected Ghanaian women. BMC Cancer 2017;17:688.ArticlePubMedPMC
- 38. Ezechi OC, Ostergren PO, Nwaokorie FO, Ujah IA, Odberg Pettersson K. The burden, distribution and risk factors for cervical oncogenic human papilloma virus infection in HIV positive Nigerian women. Virol J 2014;11:5.ArticlePubMedPMC
- 39. Kelly HA, Ngou J, Chikandiwa A, Sawadogo B, Gilham C, Omar T, et al. Associations of human papillomavirus (HPV) genotypes with high-grade cervical neoplasia (CIN2+) in a cohort of women living with HIV in Burkina Faso and South Africa. PLoS One 2017;12:e0174117.ArticlePubMedPMC
- 40. Guthrie BL, Rositch AF, Cooper JA, Farquhar C, Bosire R, Choi R, et al. Human papillomavirus and abnormal cervical lesions among HIV-infected women in HIV-discordant couples from Kenya. Sex Transm Infect 2020;96:457-463.ArticlePubMed
- 41. McDonald AC, Tergas AI, Kuhn L, Denny L, Wright TC Jr. Distribution of human papillomavirus genotypes among HIV-positive and HIV-negative women in Cape Town, South Africa. Front Oncol 2014;4:48.ArticlePubMedPMC
- 42. Adebamowo SN, Olawande O, Famooto A, Dareng EO, Offiong R, Adebamowo CA, et al. Persistent low-risk and high-risk human papillomavirus infections of the uterine cervix in HIV-negative and HIV-positive women. Front Public Health 2017;5:178.ArticlePubMedPMC
- 43. Houlihan CF, Larke NL, Watson-Jones D, Smith-McCune KK, Shiboski S, Gravitt PE, et al. Human papillomavirus infection and increased risk of HIV acquisition. A systematic review and meta-analysis. AIDS 2012;26:2211-2222.ArticlePubMed
- 44. Lissouba P, Van de Perre P, Auvert B. Association of genital human papillomavirus infection with HIV acquisition: a systematic review and meta-analysis. Sex Transm Infect 2013;89:350-356.ArticlePubMed
- 45. Auvert B, Marais D, Lissouba P, Zarca K, Ramjee G, Williamson AL. High-risk human papillomavirus is associated with HIV acquisition among South African female sex workers. Infect Dis Obstet Gynecol 2011;2011:692012.ArticlePubMedPMC
- 46. Smith-McCune KK, Shiboski S, Chirenje MZ, Magure T, Tuveson J, Ma Y, et al. Type-specific cervico-vaginal human papillomavirus infection increases risk of HIV acquisition independent of other sexually transmitted infections. PLoS One 2010;5:e10094.ArticlePubMedPMC
- 47. Namujju PB, Waterboer T, Banura C, Muwonge R, Mbidde EK, Byaruhanga R, et al. Risk of seropositivity to multiple oncogenic human papillomavirus types among human immunodeficiency virus-positive and -negative Ugandan women. J Gen Virol 2011;92:2776-2783.ArticlePubMed
REFERENCES
Figure & Data
References
Citations
- Human Papillomavirus Types and Cervical Cancer Screening among Female Sex Workers in Cameroon
Simon M. Manga, Yuanfan Ye, Kathleen L. Nulah, Florence Manjuh, Joel Fokom-Domgue, Isabel Scarinci, Alan N. Tita
Cancers.2024; 16(2): 243. CrossRef - Fighting cervical cancer in Africa: Taking a closer look at human papillomavirus 35
Sophia U. Okeke
African Journal of Laboratory Medicine.2024;[Epub] CrossRef - HIV status and knowledge of cervical cancer among women in Ghana
Nancy Innocentia Ebu Enyan, Sebastian Ken-Amoah, Derek Anamaale Tuoyire, Kafui Patrick Akakpo, Elizabeth Agyare, Dorcas Obiri-Yeboah
BMC Women's Health.2024;[Epub] CrossRef - The role of multiple high‐risk human papillomavirus infection on the persistence recurrence of high‐grade cervical lesions after standard treatment: A systematic review and a meta‐analysis
Chiara Cassani, Mattia Dominoni, Marianna Francesca Pasquali, Barbara Gardella, Arsenio Spinillo
Acta Obstetricia et Gynecologica Scandinavica.2024; 103(6): 1028. CrossRef - Prevalence of high-risk human papillomavirus genotypes in outpatient Malian women living with HIV: a pilot study
Ban Traore, Yaya Kassogue, Brehima Diakite, Fousseyni Diarra, Kadidiatou Cisse, Oumar Kassogue, Modibo Diarra, Aissata Coulibaly, Bourama Coulibaly, Hama Diallo, Zoumana Diarra, Madani Ly, Aminata Maiga, Sidi Boula Sissoko, Adama Seydou Sissoko, Cheick Bo
BMC Infectious Diseases.2024;[Epub] CrossRef - Prevalence and risk factors associated with high-risk human papillomavirus infection among women living with HIV (WLWH) at a tertiary health facility in Accra, Ghana
Frederick Agyare Gyane, Emefa Modey, Ernest Maya, Evelyn Yayra Bonney, Araba Abaidoo-Myles, Elijah Paintsil, Kwasi Torpey, Nicola Serra
PLOS ONE.2024; 19(5): e0303535. CrossRef - PD-L1 expression in squamous cervical carcinomas of Mozambican women living with or without HIV
Lucília Lovane, Satish Tulsidás, Carla Carrilho, Christina Karlsson
Scientific Reports.2024;[Epub] CrossRef - Cost-effectiveness of approaches to cervical cancer screening in Malawi: comparison of frequencies, lesion treatment techniques, and risk-stratified approaches
Petra W. Rasmussen, Risa M. Hoffman, Sam Phiri, Amos Makwaya, Gerald F. Kominski, Roshan Bastani, Agnes Moses, Corrina Moucheraud
BMC Health Services Research.2024;[Epub] CrossRef - Multiple human papillomavirus infection and high-grade cervical squamous intraepithelial lesions among women with human immunodeficiency virus: a systematic review and a meta-analysis
Chiara Cassani, Mattia Dominoni, Marianna Francesca Pasquali, Barbara Gardella, Arsenio Spinillo
Frontiers in Medicine.2024;[Epub] CrossRef - Comparison of human papillomavirus‐based cervical cancer screening strategies in Tanzania among women with and without HIV
Crispin Kahesa, Louise T. Thomsen, Ditte S. Linde, Bariki Mchome, Johnson Katanga, Patricia Swai, Rachel Manongi, Myassa Kjaerem, Thomas Iftner, Marianne Waldstrøm, Julius Mwaiselage, Vibeke Rasch, Susanne K. Kjær
International Journal of Cancer.2023; 152(4): 686. CrossRef - Human papillomavirus testing using existing nucleic acid testing platforms to screen women for cervical cancer: implementation studies from five sub-Saharan African countries
Jessica Joseph, Owen Demke, Lola Ameyan, Joseph Bitilinyu-Bango, Blandine Bourgoin, Mamadou Diop, Babacar Guèye, Jibrin Kama, Marvin Lubega, Bernard Madzima, Tatenda Maparo, Tasimba Mhizha, Andrew Musoke, Susan Nabadda, Twambilire Phiri, Timothy Tchereni,
BMJ Open.2023; 13(1): e065074. CrossRef - Utilizing first void urine for high-risk HPV testing for cervical cancer screening in HIV-positive women in Katete, Zambia
Marian Kaoma, Oladapo Olayemi, Mwila Hilton Mwaba, Kapembwa Sikwewa
BMC Women's Health.2023;[Epub] CrossRef - High-risk human papillomavirus genotype distribution among women living with and at risk for HIV in Africa
Mkunde Chachage, Ajay P. Parikh, Anifrid Mahenge, Emmanuel Bahemana, Jonathan Mnkai, Wilbert Mbuya, Ruby Mcharo, Lucas Maganga, Jaqueline Mwamwaja, Reginald Gervas, Hannah Kibuuka, Jonah Maswai, Valentine Singoei, Michael Iroezindu, Abiola Fasina, Allahna
AIDS.2023; 37(4): 625. CrossRef - The state of human papillomavirus research in Africa
Kehinde Kazeem Kanmodi, Eyinade Adeduntan Egbedina, Jimoh Amzat, Kafayat Aminu, Lawrence Achilles Nnyanzi
Public Health Challenges.2023;[Epub] CrossRef - Measuring the impact of COVID-19 social distancing measures on sexual health behaviours and access to HIV and sexual and reproductive health services for people living with HIV in Botswana
Samuel Ensor, Imogen Mechie, Rebecca Ryan, Aamirah Mussa, Bame Bame, Lefhela Tamuthiba, Neo Moshashane, Chelsea Morroni
Frontiers in Global Women's Health.2023;[Epub] CrossRef - Malignancy and viral infections in Sub-Saharan Africa: A review
Mahamadou Diakite, Kathryn Shaw-Saliba, Chuen-Yen Lau
Frontiers in Virology.2023;[Epub] CrossRef - Cervicovaginal Microbiota Profiles in Precancerous Lesions and Cervical Cancer among Ethiopian Women
Brhanu Teka, Kyoko Yoshida-Court, Ededia Firdawoke, Zewditu Chanyalew, Muluken Gizaw, Adamu Addissie, Adane Mihret, Lauren E. Colbert, Tatiana Cisneros Napravnik, Molly B. El Alam, Erica J. Lynn, Melissa Mezzari, Jhingran Anuja, Eva Johanna Kantelhardt, A
Microorganisms.2023; 11(4): 833. CrossRef - High-risk human papillomavirus genotype distribution among women living with HIV; implication for cervical cancer prevention in a resource limited setting
Patrick Kafui Akakpo, Sebastian Ken-Amoah, Nancy Innocentia Ebu Enyan, Elizabeth Agyare, Emmanuel Salia, Ibrahim Baidoo, Leonard Derkyi-Kwarteng, Matthew Asare, George Adjei, Stephen Ayisi Addo, Dorcas Obiri-Yeboah
Infectious Agents and Cancer.2023;[Epub] CrossRef - Prevalence and genotype distribution of human papillomavirus infection among women in Jingzhou, China: a population-based study of 51,720 women
Shun Liu, Bing Mei, Yaoling Ouyang, Chengbin Li
Virology Journal.2023;[Epub] CrossRef - HPV prevalence among young adult women living with and without HIV in Botswana for future HPV vaccine impact monitoring
Nancy McClung, Anikie Mathoma, Julia W. Gargano, Naledi Gape Nyepetsi, Troy D. Querec, Juanita Onyekwuluje, Madisa Mine, Chelsea Morroni, Rebecca Luckett, Lauri E. Markowitz, Doreen Ramogola-Masire
BMC Infectious Diseases.2022;[Epub] CrossRef - Acting on the call for cervical cancer elimination: Planning tools for low- and middle- income countries to increase the coverage and effectiveness of screening and treatment
Tara Herrick, Kerry A. Thomson, Michelle Shin, Sarah Gannon, Vivien Tsu, Silvia de Sanjosé
BMC Health Services Research.2022;[Epub] CrossRef - The preference of women living with HIV for the HPV self-sampling of urine at a rural HIV clinic in Uganda
Agnes Nyabigambo, Roy W. Mayega, Hilbert Mendoza, Aslam Shiraz, John Doorbar, Lynn Atuyambe, Themba G. Ginindza
Southern African Journal of Infectious Diseases.2022;[Epub] CrossRef - Cervical cancer prevention and control in women living with human immunodeficiency virus
Philip E. Castle, Mark H. Einstein, Vikrant V. Sahasrabuddhe
CA: A Cancer Journal for Clinicians.2021; 71(6): 505. CrossRef - Exogenous Vimentin Supplementation Transiently Affects Early Steps during HPV16 Pseudovirus Infection
Sinead Carse, Dirk Lang, Arieh A. Katz, Georgia Schäfer
Viruses.2021; 13(12): 2471. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite