
Articles
- Page Path
- HOME > Epidemiol Health > Volume 45; 2023 > Article
-
Original Article
Adherence to the World Cancer Research Fund/American Institute for Cancer Research and Korean Cancer Prevention Guidelines and cancer risk: a prospective cohort study from the Health Examinees-Gem study -
Jeeyoo Lee1
 , Aesun Shin1,2,3,4,5, Woo-Kyoung Shin1,4, Ji-Yeob Choi2,6,7, Daehee Kang1,2,4, Jong-Koo Lee8
, Aesun Shin1,2,3,4,5, Woo-Kyoung Shin1,4, Ji-Yeob Choi2,6,7, Daehee Kang1,2,4, Jong-Koo Lee8 -
Epidemiol Health 2023;45:e2023070.
DOI: https://doi.org/10.4178/epih.e2023070
Published online: August 1, 2023
1Department of Preventive Medicine, Seoul National University College of Medicine, Seoul, Korea
2Cancer Research Institute, Seoul National University, Seoul, Korea
3Interdisciplinary Program in Cancer Biology Major, Seoul National University College of Medicine, Seoul, Korea
4Integrated Major in Innovative Medical Science, Seoul National University Graduate School, Seoul, Korea
5Medical Research Center, Genomic Medicine Institute, Seoul National University College of Medicine, Seoul, Korea
6Department of Biomedical Science, Seoul National University Graduate School, Seoul, Korea
7Institute of Health Policy and Management, Seoul National University Medical Research Center, Seoul, Korea
8JW LEE Center for Global Medicine, Seoul National University College of Medicine, Seoul, Korea
- Correspondence: Aesun Shin Department of Preventive Medicine, Seoul National University College of Medicine, 103 Daehak-ro, Jongno-gu, Seoul 03080, Korea E-mail: shinaesun@snu.ac.kr
© 2023, Korean Society of Epidemiology
This is an open-access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
OBJECTIVES
- The purpose of this study was to explore the association between adherence to 2 cancer prevention recommendations and cancer risk.
-
METHODS
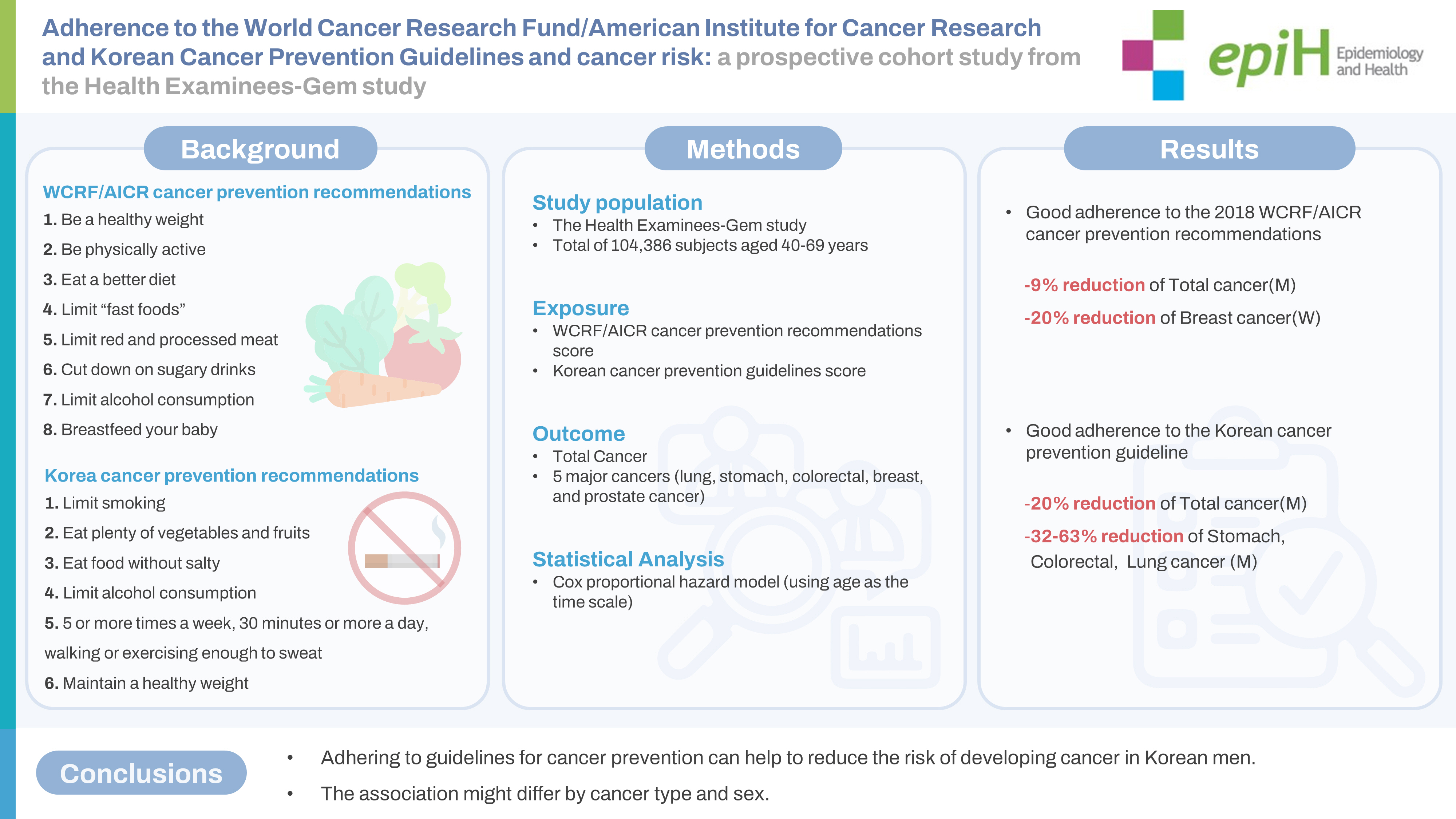
- In total, 104,386 individuals aged 40-69 years old who were recruited between 2004 and 2013 in the Health Examinees-Gem study were included. Adherence scores were constructed based on 8 items from the World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) cancer prevention recommendations, including body weight, physical activity, diet, alcohol consumption and breastfeeding, and on 6 items from the Korean cancer prevention guidelines (smoking status, eating vegetables and fruits, salty foods, alcohol intake, physical activity, and body weight). A Cox proportional hazards model was used to estimate the associations between adherence scores and the risk of total and 5 major cancers.
-
RESULTS
- The multivariable hazard ratio (HR) for total cancer with the high adherence score versus the lowest score (4.25-7.00 vs. 0.00-3.25) for the WCRF/AICR guidelines was 0.91 (95% confidence interval [CI], 0.82 to 1.00) in men. A reduced breast cancer risk was observed among women with the highest score. Men within the highest category of the Korean cancer prevention guideline score (3.25-6.00) had an HR of 0.80 (95% CI, 0.73 to 0.88) for developing total cancer compared to men within the lowest score (0.00-2.50). The higher adherence group among men showed lower risks of developing stomach, colorectal, and lung cancers.
-
CONCLUSIONS
- Adhering to guidelines for cancer prevention can help to reduce the risk of developing cancer in Korean men. The association might differ by cancer type and gender.
- Previous studies have shown that many aspects of cancer pathogenesis are related to lifestyle factors, including dietary habits [1]. It has also been reported that 30-50% of cancer cases worldwide can be prevented [2]. Countries and organizations around the world have published guidelines for cancer prevention. Among them, the recommendations for cancer prevention were updated in 2018 by the World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) based on a comprehensive literature review by expert panels [1]. Other examples are the American Cancer Society guidelines [3] in the United States, the European Code [4] in Europe, 6 cancer prevention recommendations proposed in Japan [5]. and 10 cancer prevention recommendations in the Korea [6].
- In 2018, the WCRF/AICR updated their cancer prevention guidelines, revising the recommendations made in 2007 [1]. The revised guidelines consist of 10 key points: (1) maintain a healthy weight; (2) engage in regular physical activity; (3) eat a better diet; (4) limit “fast foods”; (5) limit “consumption of red and processed meats”; (6) limit alcohol consumption; (7) cut down on sugary drinks; (8) breastfeed one’s baby if possible; (9) avoid using supplements; and (10) adhere to recommendations after a cancer diagnosis. These guidelines primarily focus on dietary habits, nutrition, and physical activity. However, they do not address other significant modifiable factors such as cigarette smoking or sun exposure. In Korea, national cancer prevention regulations and practice guidelines were established and disseminated in 2006, in line with the Cancer Prevention and Management Act, and were subsequently updated in 2016 [6]. According to the literature, there are 10 key factors for cancer prevention: smoking, consumption of vegetables and fruits, eat food without, alcohol consumption, physical activity, weight management, vaccination, sexual health, occupational safety, and cancer screening. Of these 10 factors, 4 are related to dietary habits, compared to the 6 dietary-related factors in the WCRF/AICR guidelines. Notably, the Korean guidelines include smoking, which is absent from the WCRF/AICR guidelines. Therefore, it would be intriguing to investigate the association between cancer risk and these 2 sets of guidelines within the same population.
- A previous study found that strict adherence to the 2018 WCRF/AICR cancer prevention recommendations reduced the risk of total cancer [7] and mortality [8]. An inverse association between the WCRF/AICR cancer prevention recommendations adherence score and the incidence of cancer was reported for several cancers, including colorectal cancer [9-11], pancreatic cancer [12], prostate cancer [13] and breast cancer [14-16]. However, most of these studies were conducted in Western countries, such as the United States and European nations, and no studies have investigated these issues in Asia. In Korea, prospective studies have been conducted on individual factors of cancer prevention recommendations, such as cigarette smoking, alcohol consumption, and obesity, in relation to cancer risk [17]; however, none of those studies comprehensively addressed guideline adherence as a whole.
- Therefore, our study aimed to determine whether adherence to the Korean cancer prevention guidelines and WCRF/AICR cancer prevention recommendations is associated with total cancer risk and the risk for 5 major cancers (lung, stomach, colorectal, breast, and prostate cancer) in the Korean population through a large-scale, population-based, prospective cohort study.
INTRODUCTION
- Study population
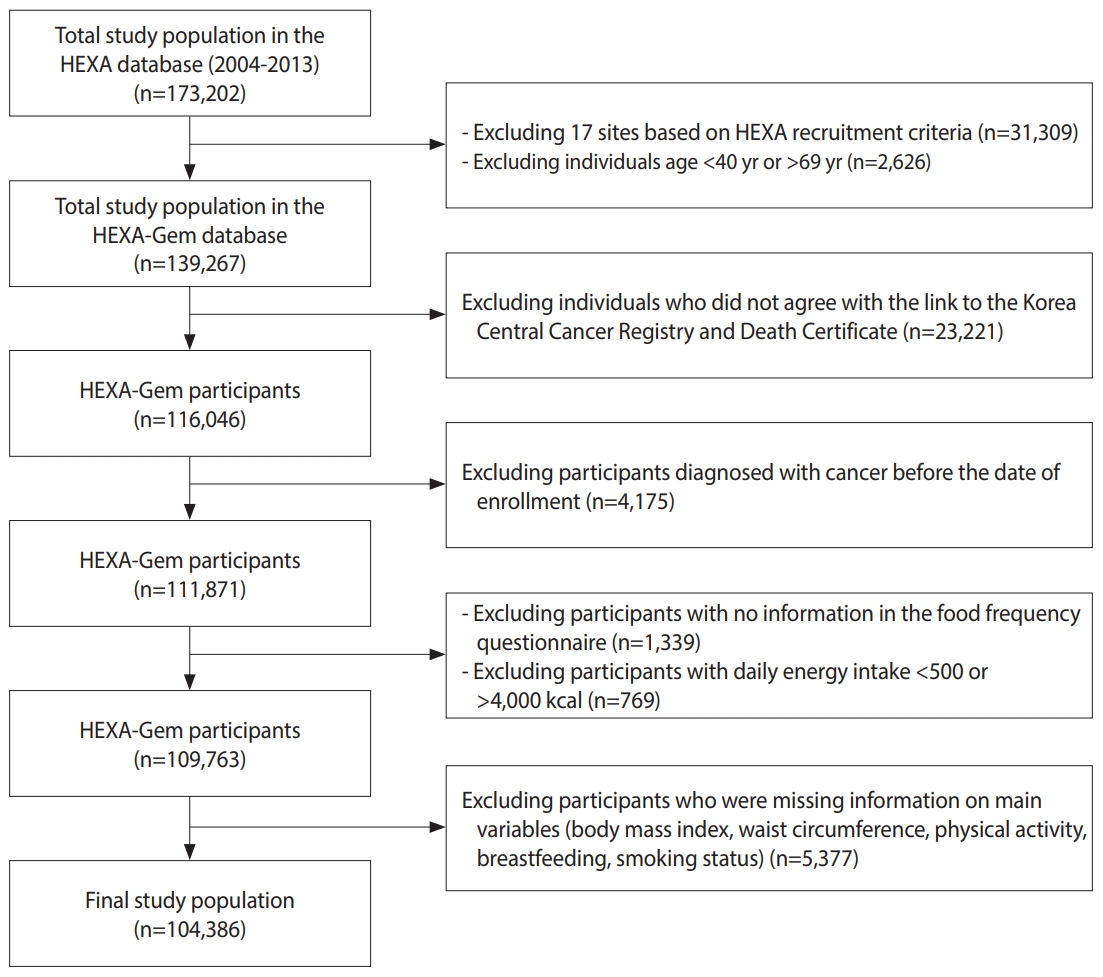
- The Health Examinees Study, a component of the Korean Genome and Epidemiology Study (KoGES) funded by the Korea Disease Control and Prevention Agency, is a large-scale population-based prospective cohort study aimed at identifying environmental and genetic factors for major chronic diseases. From 2004 to 2013, a total of 173,202 men and women were recruited from 38 hospitals and regional health check-up centers in 8 regions across Korea, selected according to a rigorous standardized research protocol. Details about the study design can be found in previous publications [18,19].
- The Health Examinees-Gem (HEXA-G) cohort was created by applying additional qualification criteria for participating organizations [20]. Of the 139,267 participants aged 40-69 years old in the HEXA-G cohort, 34,881 were excluded for the following reasons: (1) people who disagreed with linkage between the Korea Central Cancer Registry and death certificates (n=23,221); (2) people diagnosed with cancer before the date of enrollment (n=4,175); (3) those without food frequency questionnaire information (n=1,339); (4) people with daily energy intake < 500 kcal or > 4,000 kcal (n=769); and (5) people who had missing data on the main variables (body mass index [BMI], waist circumference, physical activity, breastfeeding, and smoking status) (n=5,377). The final analysis included 104,386 participants, consisting of 36,266 men and 68,130 women (Figure 1).
- World Cancer Research Fund/American Institute for Cancer Research score construction
- Information including participants’ general demographic characteristics, physical activity, lifestyle habits, and medical history was collected at baseline using structured questionnaires. For dietary information, an individual’s usual eating habits were estimated through the 106-food item semiquantitative food frequency questionnaire, which has been tested for validity and reliability [21]. Each nutrient intake and daily energy intake were calculated by the food composition table developed by the Korea Health Industry Development Institute [22].
- A standardized scoring system developed by the National Cancer Institute (NCI) of the United States and members of the AICR and WCRF International team, based on the 2018 version of the WCRF/AICR cancer prevention recommendations, was used to facilitate international comparisons between study results [23]. Eight items, excluding supplement use and recommendations for cancer survivors, constituted the proposed 2018 WCRF/AICR cancer prevention recommendations score: (1) maintain a healthy weight; (2) engage in regular physical activity; (3) eat a better diet; (4) limit fast food; (5) limit “consumption of red and processed meats”; (6) cut down on sugary drinks; (7) limit alcohol consumption; and (8) breastfeed if possible. One point was assigned to complete adherence to each recommendation, 0.5 points for partial adherence, and 0.0 points for non-adherence [23]. When there were 2 subitems, such as the healthy weight item, the score was equally divided to maintain a total of 1.0 point. According to the guidelines of the Steering Committee of the Regional Office for the Western Pacific Region of the World Health Organization [24], the BMI criterion was assigned 0.50 points if it was satisfied (18.5-22.9 kg/m2), 0.25 points if it was partially satisfied (23.0-24.9 kg/m2), and 0.00 points if it was not satisfied (< 18.5 or > 25.0 kg/m2). The waist circumference score was based on the criteria of the Korean Society for the Study of Obesity; 0.50 points were assigned if the criterion was met (men: < 90 cm, women: < 80 cm), and 0.0 points was assigned if it was not met (men: ≥ 90 cm, women: ≥ 80 cm). Details of each score component are presented in Supplementary Material 1.
- Korean cancer prevention guidelines score construction
- Among the 10 cancer prevention guidelines for Koreans, 6 items (smoking, vegetables and fruits, salty foods, alcohol, physical activity, and weight) were included in the score. For smoking, a score of 1.0 was assigned to never smokers, 0.5 to former smokers, and 0.0 to current smokers. For salty food consumption, the 2020 Dietary Reference Intakes for Koreans was used as a guide. A score of 1.0 was given for sodium intake less than 1,500 mg/day, 0.5 for intake between 1,500 mg/day and 2,300 mg/day, and 0.0 for intake of 2,300 mg/day or more [25]. The scoring for the remaining items was conducted in the same manner as the 2018 WCRF/AICR cancer prevention recommendations. Consequently, the total score for the 2018 WCRF/AICR cancer prevention recommendations, which is the aggregate of the scores for each recommendation, ranged from 0.0 points to 7.0 points for men and 0.0 points to 8.0 points for women. The Korean cancer prevention guideline score, however, had a maximum of 6.0 points for both genders. A higher score signifies greater adherence to cancer prevention recommendations. More details can be found in Supplementary Material 2.
- Ascertainment of cancer cases
- Cancer cases were ascertained through data linkage from the Korea Central Cancer Registry, which has been supervising nationwide cancer registration since 1980 under the guidance of the Ministry of Health and Welfare. Incident cases were classified as those diagnosed with cancer after the baseline survey and up until December 31, 2018.
- The top 5 major cancers were selected according to the Annual Report of Cancer Statistics in Korea in 2019 [26]. The most common cancer among Korean men and women was thyroid cancer, followed by lung cancer, stomach cancer, colorectal cancer, breast cancer, and prostate cancer. However, thyroid cancer was omitted from our selection due to the lack of identifiable preventable risk factors in comparison to the other cancers [1,27].
- Incident cancer cases were identified using the 10th revision of the International Classification of Disease, 10th revision codes C33-C34 (lung cancer), C16 (stomach cancer), C18-C20 (colorectal cancer), C50 (breast cancer), and C61 (prostate cancer).
- Statistical analysis
- Tertile score groups were used, considering the distribution of the adherence scores and examples from the previous literature [7,10,12,14,28-30]. The lowest group was analyzed as the reference group. Because the breastfeeding category only applied to women, all analyses were stratified by gender.
- Participants’ characteristics by cancer prevention recommendation score category and gender are summarized using percentages for categorical variables and means and standard deviations for continuous variables. General characteristics according to cancer prevention recommendation scores were compared using the chi-square test for categorical variables and a generalized linear model for continuous variables. The median score of each category of cancer prevention guidelines was used as a continuous variable to test for trends. The proportional hazards assumption was tested using the Schoenfeld residuals method, and no evidence of violating the assumption was found (p>0.05 for all). A Cox proportional hazards regression model was used to evaluate the associations of cancer risk with WCRF/AICR cancer prevention recommendation scores and Korean cancer prevention guideline scores. The results are presented as hazard ratios (HRs) and 95% confidence intervals (CIs). Age was chosen as the time scale [31]. The entry time was age at baseline when recruiting cohorts, and the exit time was age at the date of diagnosis of cancer, death, or the last date of follow-up (December 31, 2018), whichever came first.
- We adjusted for potential confounding variables, including education level (categorized as less than high school, high school, college or more, and missing), smoking status (divided into never smoker, ex-smoker, current smoker, and missing), total energy intake (grouped into tertiles), and family history of cancer (classified as yes, no, or missing). These variables were chosen based on previous literature. Missing data in categorical covariates were included in the multivariable Cox proportional hazards regression models as a dummy category. We estimated individual associations for each component of the WCRF/AICR cancer prevention recommendations score and the Korean Cancer Prevention Guidelines score in relation to cancer risk. To determine risk estimates and 95% CIs per 1-point increment, the WCRF/AICR cancer prevention recommendations scores and the Korean Cancer Prevention Guidelines score were also modeled as direct continuous variables. To exclude potential reverse causation due to the prevalent cancers not diagnosed at baseline, a sensitivity analysis was conducted excluding the initial 2 years of follow-up. All analyses were carried out using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
- Ethics statement
- The present study guidelines were approved by the Institutional Review Boards of the Seoul National University Hospital in Seoul, Korea (IRB No. E-2212-006-1381), and the Ethics Committee of the KoGES of the Korea National Institute of Health (IRB No. 2014-08-02-3C-A). After providing a detailed description of the study, prior written consent was collected from all participants.
MATERIALS AND METHODS
- Table 1 shows the general characteristics of the participants according to adherence to the WCRF/AICR cancer prevention recommendations. Those with high adherence tended to be older, engage in more physical activity, and consume more fruits and vegetables compared to those with low adherence. Both men and women with high adherence had lower BMI, alcohol consumption, red meat consumption, and total energy intake. The baseline characteristics for adherence to the Korean cancer prevention guidelines were largely similar to those for the WCRF/AICR cancer prevention recommendations. However, in contrast to the WCRF/AICR cancer prevention recommendations, those in the highest tertiles for adherence to the Korean cancer prevention guidelines had higher education and income levels (Supplementary Material 3).
- During a median follow-up period of 9.04 years, we identified a total of 6,987 cancer cases, comprised of 2,758 men and 4,229 women. Tables 2 and 3 display the risk of cancer in relation to the adherence score of the WCRF/AICR cancer prevention recommendation. In models adjusted for confounding factors, a high adherence score to the WCRF/AICR cancer prevention recommendations was associated with a 9% reduction in total cancer risk (HR, 0.91; 95% CI, 0.82 to 1.00) in men. A high adherence score to the Korean cancer prevention guidelines was associated with a reduced risk of total cancer (HR, 0.80; 95% CI, 0.73 to 0.88), stomach cancer (HR, 0.68; 95% CI, 0.54 to 0.84), colorectal cancer (HR, 0.74; 95% CI, 0.58 to 0.95), and lung cancer (HR, 0.37; 95% CI, 0.27 to 0.51) in men. In women, no association was found between total cancer and other types of cancer, but an inverse association was observed with breast cancer (HR, 0.80; 95% CI, 0.67 to 0.95). However, for stomach cancer in women, the risk increased by 13% for each 1-point increase in the WCRF/AICR cancer prevention recommendation score (HR, 1.13; 95% CI, 1.02 to 1.25)
- Table 4 and Supplementary Materials 4 and 5 present the associations between cancer risk and adherence to the individual components of the cancer prevention guideline score. The group with normal weight exhibited a 12% (HR, 0.88; 95% CI, 0.81 to 0.97) reduction in total cancer risk for men and a 10% (HR, 0.90; 95% CI, 0.83 to 0.96) reduction for women, compared to the underweight or obese group. Participants who met the optimal criteria for abdominal obesity (men: < 90 cm, women: < 80 cm) demonstrated a 13% (HR, 0.87; 95% CI, 0.81 to 0.95) decrease in total cancer risk for men and a 12% (HR, 0.88; 95% CI, 0.81 to 0.94) decrease for women, compared to those with abdominal obesity (men: ≥ 90 cm, women: ≥ 80 cm). Our findings also revealed that men who have never smoked had a 27% (HR, 0.73; 95% CI, 0.66 to 0.81) reduction in total cancer risk compared to current smokers.
- In a sensitivity analysis, we examined data from 35,659 men and 67,112 women, excluding the first 2 years of follow-up (Supplementary Materials 6 and 7). The findings were generally similar to the results from the main analysis. In the main analysis, women who scored highly on the WCRF/AICR cancer prevention recommendation adherence scale demonstrated a 20% decrease in breast cancer risk. However, this association was not significant in the sensitivity analysis. Conversely, women who scored highly on the Korean cancer prevention guideline scale exhibited a 25% decrease in colorectal cancer risk in the sensitivity analysis (HR, 0.75; 95% CI, 0.57 to 0.98).
RESULTS
- In this large-scale, prospective cohort study involving the Korean population, we found an inverse association between total cancer incidence and adherence to the WCRF/AICR cancer prevention guidelines among men. The Korean cancer prevention guidelines also showed an inverse association with adherence scores for total cancer, stomach cancer, colorectal cancer, and lung cancer. In women, only breast cancer showed an inverse association with adherence to the WCRF/AICR cancer prevention recommendations.
- No studies have yet explored the association between cancer risk and adherence to the 2007 or 2018 versions of the WCRF/AICR cancer prevention recommendations in Asian countries. Furthermore, the effectiveness of Korean cancer prevention guidelines remains unexamined. However, research has been conducted on the association between adherence to the 2007 version of the WCRF/AICR cancer prevention recommendations and cancer risk within the European population [7,32]. Despite variations in scoring systems, items, and racial and population characteristics, numerous studies have consistently reported that adherence to cancer prevention guidelines can help prevent cancer. Our findings align with these studies. Higher adherence to the WCRF/AICR cancer prevention recommendations was associated with a reduced risk of total cancer in the United States [33] and Sweden [7], breast cancer in Europe [14,16] and South Africa [15], and colorectal cancer in Spain [9] and the United States [10,11].
- Among the individual factors of the WCRF/AICR cancer prevention recommendations and Korean cancer prevention guidelines, strong adherence to weight management and smoking was associated with a decrease in cancer risk. Previous studies have identified obesity [34] and smoking [35] as significant risk factors among many for various types of cancer. Aside from obesity and smoking, no significant association was found with cancer risk with other individual components of the cancer prevention recommendation score.
- There were no observed associations between adherence to Korean cancer prevention guidelines and total cancers and 5 types of cancer in women. Similarly, no associations were found with other types of cancer in the WCRF/AICR cancer prevention recommendations, with the exception of breast cancer. Case-control studies conducted in South Africa [15] and Italy [16] and a cohort study in Spain [14], found that a higher score on the 2018 WCRF/AICR cancer prevention recommendations was associated with a lower risk of breast cancer. This finding was corroborated by a meta-analysis [16]. Our study discovered that for women, each one-point increase in the WCRF/AICR cancer prevention recommendations score corresponded to a 13% higher risk of stomach cancer. The precise reason for this result remains unclear, but it is plausible that the high rate of Helicobacter pylori infection, which is not included in the WCRF/AICR cancer prevention recommendations, played a significant role. The International Agency for Research on Cancer (IARC) classifies H. pylori as a class 1 carcinogen [36]. The population-attributable fraction of H. pylori infection for stomach cancer was 80.3% for men and 78.7% for women in Korea [37], which is higher than in China (63%) and in European countries (20-30%) and similar to that in Japan [38]. The main risk factors for gastric cancer among Korean women, such as age, BMI, having a family history of cancer, and past smoking status, are not adequately reflected in the WCRF/AICR recommendations [39]. In this study, we found that the risk of gastric cancer increased in women who scored highly on the individual components of breastfeeding and fast food restriction. As there are no other published studies for comparison, further research is required.
- With the exception of breast cancer, our study found a reduced cancer risk only in men who adhered to the cancer prevention recommendations, while no association was found in women. A United States study similarly found a stronger inverse association for colorectal cancer in men than in women [11]. The mechanisms behind these gender differences remain unclear, but we present several potential explanations from various perspectives. One possibility is the involvement of gender hormones. Prior research has indicated that the use of exogenous hormones, such as postmenopausal hormone therapy and oral contraceptives, as well as the increase in female hormones due to pregnancy and childbirth, may help prevent the development of colorectal cancer in women [40-42]. Another potential explanation could be gender-based differences in dietary intake and eating behavior. In Korean culture, women are more likely to purchase and prepare food, which may lead to greater nutritional knowledge and a tendency towards healthier dietary choices compared to men [43,44]. Furthermore, the number of current female smokers in our study population was extremely low (less than 5%), and the percentage of current female drinkers was 31.4%, with an average ethanol intake of 6.28 g/day. Both alcohol and smoking have been identified as risk factors for several types of cancer and are included in cancer prevention guidelines. This significant disparity in alcohol and smoking habits between men and women may have influenced our results.
- Sodium is a crucial element for maintaining homeostasis and supporting various physiological functions in the body, and it is typically acquired through salt consumption [45]. Both insufficient and excessive sodium intake can lead to a range of clinical problems. Research indicates that when sodium intake drops below 700 mg/day, it is associated with elevated total cholesterol levels in the blood [46] and increased insulin resistance [47]. According to our data, 3.36% of men and 4.62% of women reported a sodium intake of less than 700 mg/day (data not shown). Some studies have suggested a connection between a preference for salty food, salt consumption, and stomach cancer [48,49], but currently, there is no precise numerical guideline for determining the appropriate sodium intake. The evidence linking low sodium intake to cancer is both scarce and difficult to establish. Consequently, the current cancer prevention recommendation aligns with the 2020 Dietary Reference Intakes for Koreans, suggesting a sodium intake of less than 1,500 mg/day. However, it is important to acknowledge that these guidelines may need to be revised as more evidence becomes available in the future.
- Our study has several limitations that should be taken into account. First, due to the absence of data, 4 out of 10 Korean cancer prevention guidelines were not included. Further research in Korea is required to incorporate these missing elements, namely: vaccination, sexual health, safety and health, and cancer screening. Second, the cancer prevention guidelines used in our study, including the Korean cancer prevention guidelines and the WCRF/AICR cancer prevention recommendations, utilized a standardized scoring system for ease of comparison. This system did not assign weights to the components, assuming all to be of equal importance. Future studies should consider the relative weights of these components and their relevance to different racial groups. Thirdly, despite adjusting for confounding factors, it is possible that some residual and unmeasured confounding factors were not eliminated. Despite these limitations, this study is significant as it is a large-scale investigation into the associations between adherence to cancer prevention guidelines, including diet, and cancer risk, a topic that has primarily been studied in the Western world. Another strength of this study is that the accuracy of cancer diagnoses was ensured by linkage to the Korea Central Cancer Registry, which contained an estimated 98.3% of data on cancer incidence in 2019 [50].
- In conclusion, these cohort study’s findings indicate that adherence to both the WCRF/AICR cancer prevention recommendations and Korean cancer prevention guidelines can prevent cancer in men. Additionally, we discovered that adherence to the WCRF/AICR cancer prevention recommendations can aid in preventing breast cancer in Korean women. The effectiveness of these guidelines may vary depending on the type of cancer and the individual’s gender. However, due to data limitations, we were unable to consider all aspects of the Korean cancer prevention guidelines. Therefore, further research is required.
DISCUSSION
SUPPLEMENTARY MATERIALS
Supplement Material 1.
Supplement Material 2.
Supplement Material 3.
Supplement Material 4.
Supplement Material 5.
Supplement Material 6.
Supplement Material 7.
-
CONFLICT OF INTEREST
The authors have no conflicts of interest to declare for this study.
-
FUNDING
This research was supported by a National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (No. 2022R1A2C1004608).
-
AUTHOR CONTRIBUTIONS
Conceptualization: Lee J, Shin A, Shin WK, Choi JY. Data curation: Lee J. Formal analysis: Lee J, Shin A. Funding acquisition: Shin A, Choi JY, Kang D, Lee JK. Methodology: Lee J, Shin A. Project administration: Lee J, Shin A, Choi JY, Kang D, Lee JK. Visualization: Lee J. Writing – original draft: Lee J, Shin A. Writing – review & editing: Lee J, Shin A, Shin WK, Choi JY, Kang D, Lee JK.
NOTES
ACKNOWLEDGEMENTS
| Characteristics |
WCRF/AICR adherence score |
||||||||
|---|---|---|---|---|---|---|---|---|---|
|
Men (n=36,266) |
Women (n=68,130) |
||||||||
| Tertile 1 | Tertile 2 | Tertile 3 | p-value1 | Tertile 1 | Tertile 2 | Tertile 3 | p-value1 | ||
| Score range | 0.00≤score<3.25 | 3.25≤score<4.25 | score≥4.25 | 0.00≤score<4.50 | 4.50≤score<5.50 | score≥5.50 | |||
| No. of participants | 10,947 (30.2) | 13,091 (36.1) | 12,228 (33.7) | <0.001 | 19,732 (29.0) | 24,186 (35.5) | 24,212 (35.5) | <0.001 | |
| Age (yr) | 50.9±8.2 | 53.4±8.3 | 56.0±7.9 | <0.001 | 49.3±7.5 | 52.5±7.7 | 54.5±7.2 | <0.001 | |
| Body mass index (kg/m2) | 25.5±2.9 | 24.4±2.7 | 23.5±2.2 | <0.001 | 24.2±3.3 | 23.7±3.0 | 23.0±2.5 | <0.001 | |
| Education | <0.001 | <0.001 | |||||||
| ≤Middle school | 1,973 (18.0) | 2,799 (21.4) | 2,554 (20.9) | 4,977 (25.2) | 9,003 (37.2) | 10,145 (41.9) | |||
| High school | 4,579 (41.8) | 5,301 (40.5) | 4,928 (40.3) | 9,018 (45.7) | 10,233 (42.3) | 10,336 (42.7) | |||
| ≥College | 4,309 (39.4) | 4,881 (37.3) | 4,623 (37.8) | 5,614 (28.5) | 4,784 (19.8) | 3,552 (14.7) | |||
| Missing | 86 (0.8) | 110 (0.8) | 123 (1.0) | 123 (0.6) | 166 (0.7) | 179 (0.7) | |||
| Income (104 Korean won) | <0.001 | <0.001 | |||||||
| <200 | 2,168 (19.8) | 3,172 (24.2) | 3,274 (26.8) | 5,003 (25.3) | 7,475 (30.9) | 7,786 (32.2) | |||
| 200-400 | 5,038 (46.0) | 5,631 (43.0) | 5,042 (41.2) | 8,257 (41.9) | 9,341 (38.6) | 9,231 (38.1) | |||
| ≥400 | 3,250 (29.7) | 3,548 (27.1) | 3,180 (26.0) | 5,320 (27.0) | 5,707 (23.6) | 5,275 (21.8) | |||
| Missing | 491 (4.5) | 740 (5.7) | 732 (6.0) | 1,152 (5.8) | 1,663 (6.9) | 1,920 (7.9) | |||
| Smoking status | <0.001 | <0.001 | |||||||
| Never | 2,366 (21.6) | 3,485 (26.6) | 3,940 (32.3) | 18,505 (93.8) | 23,428 (96.9) | 23,755 (98.1) | |||
| Former | 4,074 (37.2) | 5,291 (40.4) | 5,446 (44.5) | 409 (2.0) | 269 (1.1) | 180 (0.8) | |||
| Current | 4,507 (41.2) | 4315 (33.0) | 2,842 (23.2) | 818 (4.2) | 489 (2.0) | 277 (1.1) | |||
| Missing | |||||||||
| Alcohol intake, (g of ethanol/day) | 23.9±44.5 | 14.7±26.4 | 8.6±19.2 | <0.001 | 3.8±13.5 | 1.7±26.1 | 0.7±4.1 | <0.001 | |
| Physical activity (min/wk) | <0.001 | <0.001 | |||||||
| <75 | 8,170(74.6) | 6,635(50.7) | 2,438(19.9) | 15,863(80.3) | 14,565(60.2) | 6,016(24.9) | |||
| 75-149 | 891 (8.2) | 1,414 (10.8) | 1,060 (8.7) | 1,410 (7.2) | 2,457 (10.2) | 2,332 (9.6) | |||
| ≥150 | 1,886 (17.2) | 5,042 (38.5) | 8,730 (71.4) | 2,459 (12.5) | 7,164 (29.6) | 15,864 (65.5) | |||
| Family history of cancer | 0.618 | 0.615 | |||||||
| No | 8,049 (73.5) | 9,521 (72.7) | 8,967 (73.3) | 13,878 (70.3) | 16,951 (70.1) | 17,081 (70.5) | |||
| Yes | 2,877 (26.3) | 3,539 (27.1) | 3,233 (26.5) | 5,803 (29.4) | 7,178 (29.7) | 7,082 (29.3) | |||
| Missing | 21 (0.2) | 31 (0.2) | 28 (0.2) | 51 (0.3) | 57 (0.2) | 49 (0.2) | |||
| Breastfeeding (mo) | <0.001 | ||||||||
| None | - | - | - | 7,987 (40.5) | 3,629 (15.0) | 1,083 (4.4) | |||
| <6 | - | - | - | 2,628 (13.3) | 2,181 (9.0) | 1,151 (4.8) | |||
| ≥6 | - | - | - | 9,117 (46.2) | 18,376 (76.0) | 21,978 (90.8) | |||
| Energy intake (kcal/day) | 2,012.2±533.7 | 1,823.4±489.9 | 1,718.4±420.9 | <0.001 | 1,809.5±544.4 | 1,667.2±503.6 | 1,613.2±454.8 | <0.001 | |
| Vegetable and fruits intake (g/day) | 244.5±163.1 | 260.5±178.4 | 299.3±191.7 | <0.001 | 226.4±153 | 247±168.9 | 300.6±197.1 | <0.001 | |
| Fast food intake (g/day) | 61.7±51.7 | 40.8±44.5 | 21.9±29.8 | <0.001 | 57.8±54.6 | 35.0±43.6 | 18.1±29.4 | <0.001 | |
| Red meat intake (g/day) | 78.5±58.3 | 49.8±48.2 | 33.6±31.9 | <0.001 | 57.1±55.2 | 35.1±39.3 | 25.8±27.4 | <0.001 | |
| Sugar-sweetened drinks (g/day) | 75.0±104.7 | 54.8±78.3 | 47.2±62.1 | <0.001 | 64.8±93.0 | 54.8±75.5 | 51.3±66.7 | <0.001 | |
| Sodium intake (g/day) | 2,637.7±1,371.2 | 2,587.4±1,432.0 | 2,717.5±1,450.8 | <0.001 | 2,296.3±1,226.6 | 2,298.3±1,301.1 | 2,559.2±1,412.6 | <0.001 | |
| Variables |
Men (n=36,266) |
Women (n=68,130) |
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Tertile 1 | Tertile 2 | Tertile 3 | p for trend2 | Continuous (per 1-point increase in score) | Tertile 1 | Tertile 2 | Tertile 3 | p for trend2 | Continuous (per 1-point increase in score) | ||
| Score range | 0.00≤score<3.25 | 3.25≤score<4.25 | score≥4.25 | - | - | 0.00≤score<4.50 | 4.50≤score<5.50 | score≥5.50 | - | - | |
| Person-years | 96,520.70 | 115,445.60 | 107,406.40 | - | - | 172,867.90 | 214,532.00 | 215,386.00 | - | - | |
| Total cancer | |||||||||||
| No. of cases/total subjects | 724/10,947 | 1,000/13,091 | 1,034/12,228 | - | - | 1,173/19,732 | 1,510/24,186 | 1,546/24,212 | - | - | |
| Crude HR (95% CI) | 1.00 (reference) | 0.95 (0.86, 1.05) | 0.89 (0.80, 0.98) | 0.013 | 0.97 (0.93, 1.00) | 1.00 (reference) | 0.98 (0.91, 1.06) | 0.97 (0.89, 1.05) | 0.394 | 0.99 (0.96, 1.02) | |
| Multivariable-adjusted HR (95% CI) | 1.00 (reference) | 0.96 (0.87, 1.05) | 0.91 (0.82, 1.00) | 0.053 | 0.98 (0.94, 1.02) | 1.00 (reference) | 0.99 (0.91, 1.07) | 0.98 (0.90, 1.06) | 0.553 | 0.99 (0.96, 1.02) | |
| Stomach cancer | |||||||||||
| No. of cases/total subjects | 134/10,947 | 183/13,091 | 181/12,228 | - | - | 87/19,732 | 137/24,186 | 178/24,212 | - | - | |
| Crude HR (95% CI) | 1.00 (reference) | 0.97 (0.77, 1.21) | 0.89 (0.71, 1.12) | 0.314 | 0.95 (0.87, 1.04) | 1.00 (reference) | 1.09 (0.83, 1.43) | 1.29 (0.99, 1.69) | 0.050 | 1.14 (1.04, 1.26) | |
| Multivariable-adjusted HR (95% CI) | 1.00 (reference) | 1.00 (0.79, 1.25) | 0.95 (0.75, 1.21) | 0.651 | 0.98 (0.89, 1.08) | 1.00 (reference) | 1.07 (0.81, 1.41) | 1.26 (0.96, 1.65) | 0.080 | 1.13 (1.02, 1.25) | |
| Colorectal cancer | |||||||||||
| No. of cases/total subjects | 111/10,947 | 143/13,091 | 143/12,228 | - | - | 89/19,732 | 152/24,186 | 147/24,212 | - | - | |
| Crude HR (95% CI) | 1.00 (reference) | 0.92 (0.72, 1.18) | 0.87 (0.67, 1.11) | 0.260 | 0.93 (0.84, 1.03) | 1.00 (reference) | 1.12 (0.86, 1.46) | 0.97 (0.74, 1.27) | 0.742 | 0.97 (0.88, 1.07) | |
| Multivariable-adjusted HR (95% CI) | 1.00 (reference) | 0.90 (0.70, 1.16) | 0.83 (0.64, 1.08) | 0.161 | 0.91 (0.82, 1.02) | 1.00 (reference) | 1.14 (0.87, 1.49) | 0.99 (0.76, 1.31) | 0.864 | 0.98 (0.89, 1.08) | |
| Lung cancer | |||||||||||
| No. of cases/total subjects | 76/10,947 | 114/13,091 | 101/12,228 | - | - | 62/19,732 | 93/24,186 | 88/24,212 | - | - | |
| Crude HR (95% CI) | 1.00 (reference) | 0.95 (0.71, 1.27) | 0.70 (0.52, 0.95) | 0.015 | 0.90 (0.81, 1.00) | 1.00 (reference) | 0.89 (0.65, 1.23) | 0.73 (0.53, 1.01) | 0.047 | 0.91 (0.80, 1.03) | |
| Multivariable-adjusted HR (95% CI) | 1.00 (reference) | 1.02 (0.76, 1.37) | 0.86 (0.63, 1.18) | 0.333 | 0.99 (0.88, 1.11) | 1.00 (reference) | 0.94 (0.68, 1.30) | 0.77 (0.55, 1.07) | 0.102 | 0.93 (0.82, 1.06) | |
| Prostate (men)/Breast cancer (women) | |||||||||||
| No. of cases/total subjects | 103/10,947 | 153/13,091 | 193/12,228 | - | - | 294/19,732 | 295/24,186 | 273/24,212 | - | - | |
| Crude HR (95% CI) | 1.00 (reference) | 0.89 (0.70, 1.14) | 0.91 (0.72, 1.16) | 0.507 | 0.97 (0.88, 1.07) | 1.00 (reference) | 0.84 (0.71, 0.98) | 0.79 (0.66, 0.94) | 0.006 | 0.91 (0.85, 0.97) | |
| Multivariable-adjusted HR (95% CI) | 1.00 (reference) | 0.89 (0.69, 1.14) | 0.89 (0.70, 1.13) | 0.367 | 0.95 (0.87, 1.05) | 1.00 (reference) | 0.84 (0.71, 1.00) | 0.80 (0.67, 0.95) | 0.010 | 0.91 (0.85, 0.97) | |
HR, hazard ratio; CI, confidence interval; WCRF/AICR, World Cancer Research Fund/American Institute for Cancer Research.
1 Adjusted for education level (less than high school, high school, college or above, and missing), smoking status (non-smoker, ex-smoker, current smoker, and missing), total energy intake (tertiles), and family history of cancer (yes, no, and missing).
2 The test for trend was calculated with the median score for each category of the cancer prevention guideline as a continuous variable.
| Variables |
Men (n=36,266) |
Women (n=68,130) |
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Tertile 1 | Tertile 2 | Tertile 3 | p for trend2 | Continuous (per 1-point increase in score) | Tertile 1 | Tertile 2 | Tertile 3 | p for trend2 | Continuous (per 1-point increase in score) | ||
| Score range | 0.00≤score<2.50 | 2.50≤score<3.25 | score≥3.25 | - | - | 0.00≤score<3.50 | 3.50≤score<4.00 | score≥4.00 | - | - | |
| Person-years | 101,000.20 | 106,238.80 | 112,133.70 | - | - | 194,374.80 | 151,862.50 | 256,548.60 | - | - | |
| Total cancer | |||||||||||
| No. of cases/total subjects | 827/11,402 | 975/12,139 | 956/12,725 | - | - | 1,396/21,979 | 1,031/17,065 | 1,802/29,086 | - | - | |
| Crude HR (95% CI) | 1.00 (reference) | 0.97 (0.88, 1.06) | 0.80 (0.73, 0.88) | <0.001 | 0.90 (0.86, 0.94) | 1.00 (reference) | 0.95 (0.88, 1.03) | 0.97 (0.91, 1.05) | 0.587 | 0.98 (0.95, 1.02) | |
| Multivariable-adjusted HR (95% CI) | 1.00 (reference) | 0.97 (0.88, 1.06) | 0.80 (0.73, 0.88) | <0.001 | 0.90 (0.86, 0.94) | 1.00 (reference) | 0.94 (0.87, 1.02) | 0.96 (0.90, 1.03) | 0.407 | 0.98 (0.94, 1.02) | |
| Stomach cancer | |||||||||||
| No. of cases/total subjects | 168/11,402 | 171/12,139 | 159/12,725 | - | - | 132/21,979 | 80/17,065 | 190/29,086 | - | - | |
| Crude HR (95% CI) | 1.00 (reference) | 0.85 (0.69, 1.06) | 0.68 (0.55, 0.85) | <0.001 | 0.83 (0.75, 0.92) | 1.00 (reference) | 0.79 (0.60, 1.04) | 1.09 (0.88, 1.36) | 0.253 | 1.07 (0.94, 1.22) | |
| Multivariable-adjusted HR (95% CI) | 1.00 (reference) | 0.85 (0.69, 1.05) | 0.68 (0.54, 0.84) | <0.001 | 0.83 (0.75, 0.92) | 1.00 (reference) | 0.79 (0.59, 1.04) | 1.09 (0.87, 1.36) | 0.276 | 1.07 (0.94, 1.22) | |
| Colorectal cancer | |||||||||||
| No. of cases/total subjects | 134/11,402 | 128/12,139 | 135/12,725 | - | - | 132/21,979 | 98/17,065 | 158/29,086 | - | - | |
| Crude HR (95% CI) | 1.00 (reference) | 0.81 (0.64, 1.04) | 0.74 (0.58, 0.94) | 0.021 | 0.90 (0.81, 1.01) | 1.00 (reference) | 0.97 (0.74, 1.25) | 0.89 (0.71, 1.13) | 0.328 | 0.93 (0.81, 1.06) | |
| Multivariable-adjusted HR (95% CI) | 1.00 (reference) | 0.81 (0.64, 1.04) | 0.74 (0.58, 0.95) | 0.047 | 0.90 (0.81, 1.01) | 1.00 (reference) | 0.95 (0.73, 1.24) | 0.88 (0.69, 1.11) | 0.254 | 0.92 (0.80, 1.05) | |
| Lung cancer | |||||||||||
| No. of cases/total subjects | 111/11,402 | 114/12,139 | 66/12,725 | - | - | 89/21,979 | 48/17,065 | 106/29,086 | - | - | |
| Crude HR (95% CI) | 1.00 (reference) | 0.79 (0.60, 1.02) | 0.36 (0.27, 0.49) | <0.001 | 0.68 (0.60, 0.76) | 1.00 (reference) | 0.72 (0.50, 1.02) | 0.92 (0.69, 1.21) | 0.744 | 1.03 (0.86, 1.23) | |
| Multivariable-adjusted HR (95% CI) | 1.00 (reference) | 0.80 (0.61, 1.04) | 0.37 (0.27, 0.51) | <0.001 | 0.69 (0.61, 0.78) | 1.00 (reference) | 0.70 (0.49, 0.99) | 0.88 (0.66, 1.17) | 0.554 | 1.01 (0.84, 1.20) | |
| Prostate (men)/Breast cancer (women) | |||||||||||
| No. of cases/total subjects | 95/11,402 | 154/12,139 | 200/12,725 | - | - | 289/21,979 | 218/17,065 | 355/29,086 | - | - | |
| Crude HR (95% CI) | 1.00 (reference) | 1.20 (0.93, 1.56) | 1.22 (0.96, 1.56) | 0.154 | 1.07 (0.96, 1.19) | 1.00 (reference) | 0.96 (0.81, 1.15) | 0.93 (0.80, 1.09) | 0.389 | 0.95 (0.87, 1.04) | |
| Multivariable-adjusted HR (95% CI) | 1.00 (reference) | 1.18 (0.92, 1.53) | 1.18 (0.92, 1.51) | 0.260 | 1.05 (0.95, 1.17) | 1.00 (reference) | 0.93 (0.78, 1.11) | 0.88 (0.75, 1.04) | 0.132 | 0.92 (0.84, 1.01) | |
1 Adjusted for education level (less than high school, high school, college or above, and missing), total energy intake (tertiles), and family history of cancer (yes, no, and missing).
2 The test for trend was calculated with the median score for each category of the cancer prevention guideline as a continuous variable.
| Components of the cancer prevention guideline score |
Men (n=36,266) |
Women (n=68,130) |
|||||||
|---|---|---|---|---|---|---|---|---|---|
| No. of cases/total participants | Person-year | Crude HR (95% CI) | Multivariable-adjusted HR (95% CI) | No. of cases/total participants | Person-year | Crude HR (95% CI) | Multivariable-adjusted HR (95% CI) | ||
| Maintain a healthy weight (BMI)2,3 | |||||||||
| 0.00 | 1,198/15,038 | 132,232.10 | 1.00 (reference) | 1.00 (reference) | 1,369/20,481 | 180,210.80 | 1.00 (reference) | 1.00 (reference) | |
| 0.25 | 792/10,966 | 96,903.70 | 0.86 (0.79, 0.94) | 0.86 (0.79, 0.94) | 1,147/18,088 | 161,030.00 | 0.95 (0.88, 1.03) | 0.95 (0.88, 1.03) | |
| 0.50 | 768/10,262 | 90,236.90 | 0.89 (0.82, 0.98) | 0.88 (0.81, 0.97) | 1,713/29,561 | 261,545.10 | 0.91 (0.85, 0.98) | 0.90 (0.83, 0.96) | |
| Maintain a healthy weight (WC)2,3 | |||||||||
| 0.0 | 921/10,506 | 92,990.00 | 1.00 (reference) | 1.00 (reference) | 1,003/13,984 | 124,309.40 | 1.00 (reference) | 1.00 (reference) | |
| 0.5 | 1,837/25,760 | 226,382.70 | 0.87 (0.81, 0.94) | 0.87 (0.81, 0.95) | 3,226/54,146 | 478,476.50 | 0.89 (0.83, 0.96) | 0.88 (0.81, 0.94) | |
| Be physically active2,3 | |||||||||
| 0.0 | 1,293/17,243 | 153,028.70 | 1.00 (reference) | 1.00 (reference) | 2,232/36,444 | 324,485.80 | 1.00 (reference) | 1.00 (reference) | |
| 0.5 | 229/3,365 | 30,058.30 | 0.97 (0.85, 1.12) | 1.01 (0.87, 1.16) | 386/6,199 | 55,514.50 | 1.01 (0.91, 1.13) | 1.00 (0.90, 1.12) | |
| 1.0 | 1,236/15,658 | 136,285.80 | 0.94 (0.87, 1.02) | 0.98 (0.90, 1.06) | 1,611/25,487 | 222,785.50 | 1.04 (0.97, 1.11) | 1.03 (0.97, 1.10) | |
| Eat a better diet2,3 | |||||||||
| 0.0 | 1,115/14,175 | 124,235.30 | 1.00 (reference) | 1.00 (reference) | 1,762/28,614 | 250,984.80 | 1.00 (reference) | 1.00 (reference) | |
| 0.5 | 1,203/16,220 | 142,456.70 | 0.96 (0.88, 1.04) | 0.96 (0.88, 1.04) | 1,849/29,557 | 260,334.70 | 1.01 (0.95, 1.08) | 1.01 (0.94, 1.08) | |
| 1.0 | 440/5,871 | 52,680.80 | 0.96 (0.86, 1.08) | 0.97 (0.87, 1.10) | 618/9,959 | 91,466.30 | 0.96 (0.88, 1.05) | 0.95 (0.87, 1.05) | |
| Limit fast foods2 | |||||||||
| 0.0 | 719/12,078 | 106,275.40 | 1.00 (reference) | 1.00 (reference) | 1,329/22,675 | 200,205.80 | 1.00 (reference) | 1.00(reference) | |
| 0.5 | 927/12,158 | 106,979.00 | 1.09 (0.99, 1.20) | 1.08 (0.98, 1.20) | 1,400/22808 | 201,475.80 | 1.00 (0.93, 1.08) | 1.01 (0.94, 1.10) | |
| 1.0 | 1,112/12,030 | 106,118.40 | 1.05 (0.95, 1.15) | 1.04 (0.94, 1.16) | 1,500/22,647 | 201,104.30 | 1.01 (0.94, 1.09) | 1.04 (0.96, 1.13) | |
| Limit red and processed meat2 | |||||||||
| 0.0 | 580/8,857 | 78,183.60 | 1.00 (reference) | 1.00 (reference) | 587/9,901 | 86,949.20 | 1.00 (reference) | 1.00 (reference) | |
| 0.5 | 83/1,975 | 17,114.30 | 0.85 (0.68, 1.07) | 0.85 (0.67, 1.07) | 194/3,643 | 31,001.70 | 0.99 (0.84, 1.17) | 0.99 (0.84, 1.16) | |
| 1.0 | 2,095/25,434 | 224,074.90 | 1.04 (0.95, 1.14) | 1.05 (0.95, 1.16) | 3,448/54,586 | 484,835.00 | 1.01 (0.92, 1.10) | 1.01 (0.92, 1.11) | |
| Cut down on sugary drinks2 | |||||||||
| 0.0 | 97/1,393 | 12,506.20 | 1.00 (reference) | 1.00 (reference) | 137/2,303 | 21,171.20 | 1.00 (reference) | 1.00 (reference) | |
| 0.5 | 2,601/34,352 | 302,363.00 | 0.92 (0.75, 1.13) | 0.90 (0.73, 1.11) | 4,043/64,961 | 573,944.50 | 1.07 (0.90, 1.27) | 1.08 (0.91, 1.29) | |
| 1.0 | 60/521 | 4,503.50 | 1.22 (0.88, 1.69) | 1.18 (0.85, 1.64) | 49/866 | 7,670.20 | 0.93 (0.67, 1.29) | 0.96 (0.69, 1.33) | |
| Limit alcohol consumption2,3 | |||||||||
| 0.0 | 469/6,442 | 56,408.00 | 1.00 (reference) | 1.00 (reference) | 120/2,224 | 19,311.50 | 1.00 (reference) | 1.00 (reference) | |
| 0.5 | 1,405/19,788 | 174,640.80 | 0.88 (0.79, 0.97) | 0.91 (0.81, 1.01) | 1,063/18,455 | 162,073.20 | 1.04 (0.86, 1.26) | 1.04 (0.86, 1.26) | |
| 1.0 | 884/10,036 | 88,323.90 | 0.93 (0.83, 1.04) | 0.99 (0.88, 1.11) | 3,046/47,451 | 421,401.20 | 1.07 (0.89, 1.29) | 1.07 (0.89, 1.30) | |
| For mothers: breastfeed your baby2 | |||||||||
| 0.0 | - | - | - | - | 762/12,699 | 110,432.50 | 1.00 (reference) | 1.00 (reference) | |
| 0.5 | - | - | - | - | 319/5,960 | 52,663.30 | 0.90 (0.79, 1.03) | 0.90 (0.79, 1.02) | |
| 1.0 | - | - | - | - | 3,148/49,471 | 439,690.10 | 0.96 (0.88, 1.04) | 0.98 (0.90, 1.07) | |
| Limit smoking3,4 | |||||||||
| 0.0 | 864/11,664 | 102,415.50 | 1.00 (reference) | 1.00 (reference) | 94/1,584 | 13,646.70 | 1.00 (reference) | 1.00 (reference) | |
| 0.5 | 1,191/14,811 | 129,113.40 | 0.81 (0.74, 0.89) | 0.81 (0.74, 0.89) | 53/858 | 7,503.90 | 1.01 (0.72, 1.41) | 1.00 (0.71, 1.39) | |
| 1.0 | 703/9,791 | 87,843.80 | 0.73 (0.66, 0.80) | 0.73 (0.66, 0.81) | 4,082/65,688 | 581,635.30 | 0.97 (0.79, 1.19) | 0.96 (0.78, 1.18) | |
| Eat food without salty (sodium intake)3 | |||||||||
| 0.0 | 1,470/20,060 | 178,067.60 | 1.00 (reference) | 1.00 (reference) | 2,010/31,956 | 157,922.30 | 1.00 (reference) | 1.00 (reference) | |
| 0.5 | 675/8,784 | 76,092.30 | 1.03 (0.94, 1.13) | 1.03 (0.94, 1.13) | 1,090/18,236 | 286,165.80 | 0.98 (0.91, 1.05) | 0.98 (0.91, 1.06) | |
| 1.0 | 613/7,422 | 65,212.80 | 1.04 (0.95, 1.14) | 1.04 (0.94, 1.16) | 1,129/17,938 | 158,697.80 | 1.01 (0.94, 1.08) | 1.01 (0.94, 1.10) | |
HR, hazard ratio; CI, confidence interval; BMI, body mass index; WC, waist circumference; WCRF/AICR, World Cancer Research Fund/American Institute for Cancer Research.
1 Adjusted for education level (less than high school, high school, college or above, and missing), smoking status (non-smoker, ex-smoker, current smoker, and missing), total energy intake (tertiles), and family history of cancer (yes, no, and missing).
2 Components of the WCRF/AICR score.
3 Components of the Korean Cancer Prevention Guidelines score.
4 Adjusted for education level (less than high school, high school, college or above, and missing), total energy intake (tertiles), and family history of cancer (yes, no, and missing).
- 1. World Cancer Research Fund/American Institute for Cancer Research. Diet, nutrition, physical activity and cancer: a global perspective: a summary of the third expert repot; 2018 [cited 2022 Sep 19]. Available from: https://www.wcrf.org/wp-content/uploads/2021/02/Summary-of-Third-Expert-Report-2018.pdf.
- 2. Doll R, Peto R. The causes of cancer: quantitative estimates of avoidable risks of cancer in the United States today. J Natl Cancer Inst 1981;66:1191-1308.ArticlePubMed
- 3. Rock CL, Thomson C, Gansler T, Gapstur SM, McCullough ML, Patel AV, et al. American cancer society guideline for diet and physical activity for cancer prevention. CA Cancer J Clin 2020;70:245-271.ArticlePubMedPDF
- 4. Schüz J, Espina C, Villain P, Herrero R, Leon ME, Minozzi S, et al. European Code against cancer 4th edition: 12 ways to reduce your cancer risk. Cancer Epidemiol 2015;39 Suppl 1:S1-S10.PubMed
- 5. Sasazuki S, Inoue M, Shimazu T, Wakai K, Naito M, Nagata C, et al. Evidence-based cancer prevention recommendations for Japanese. Jpn J Clin Oncol 2018;48:576-586.ArticlePubMed
- 6. Ministry of Health and Welfare. Press release: avoid alcohol consumption! Get vaccine for cancer prevention!; 2016 [cited 2022 Sep 19]. Available from: http://www.mohw.go.kr/react/al/sal0301vw.jsp?PAR_MENU_ID=04&MENU_ID=0403&CONT_SEQ=330589 (Korean).
- 7. Kaluza J, Harris HR, Håkansson N, Wolk A. Adherence to the WCRF/AICR 2018 recommendations for cancer prevention and risk of cancer: prospective cohort studies of men and women. Br J Cancer 2020;122:1562-1570.ArticlePubMedPMCPDF
- 8. Shams-White MM, Brockton NT, Mitrou P, Kahle LL, Reedy J. The 2018 World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) score and all-cause, cancer, and cardiovascular disease mortality risk: a longitudinal analysis in the NIH-AARP Diet and Health Study. Curr Dev Nutr 2022;6:nzac096.ArticlePubMedPMCPDF
- 9. Barrubés L, Babio N, Hernández-Alonso P, Toledo E, Ramírez Sabio JB, Estruch R, et al. Association between the 2018 WCRF/AICR and the low-risk lifestyle scores with colorectal cancer risk in the PREDIMED study. J Clin Med 2020;9:1215.ArticlePubMedPMC
- 10. Onyeaghala G, Lintelmann AK, Joshu CE, Lutsey PL, Folsom AR, Robien K, et al. Adherence to the World Cancer Research Fund/American Institute for Cancer Research cancer prevention guidelines and colorectal cancer incidence among African Americans and whites: the Atherosclerosis Risk in Communities study. Cancer 2020;126:1041-1050.ArticlePubMedPDF
- 11. Petimar J, Smith-Warner SA, Rosner B, Chan AT, Giovannucci EL, Tabung FK. Adherence to the World Cancer Research Fund/American Institute for Cancer Research 2018 recommendations for cancer prevention and risk of colorectal cancer. Cancer Epidemiol Biomarkers Prev 2019;28:1469-1479.ArticlePubMedPMCPDF
- 12. Zhang ZQ, Li QJ, Hao FB, Wu YQ, Liu S, Zhong GC. Adherence to the 2018 World Cancer Research Fund/American Institute for Cancer Research cancer prevention recommendations and pancreatic cancer incidence and mortality: a prospective cohort study. Cancer Med 2020;9:6843-6853.ArticlePubMedPMCPDF
- 13. Olmedo-Requena R, Lozano-Lorca M, Salcedo-Bellido I, Jiménez-Pacheco A, Vázquez-Alonso F, García-Caballos M, et al. Compliance with the 2018 World Cancer Research Fund/American Institute for Cancer Research cancer prevention recommendations and prostate cancer. Nutrients 2020;12:768.ArticlePubMedPMC
- 14. Barrios-Rodríguez R, Toledo E, Martinez-Gonzalez MA, Aguilera-Buenosvinos I, Romanos-Nanclares A, Jiménez-Moleón JJ. Adherence to the 2018 World Cancer Research Fund/American Institute for Cancer Research recommendations and breast cancer in the SUN Project. Nutrients 2020;12:2076.ArticlePubMedPMC
- 15. Jacobs I, Taljaard-Krugell C, Wicks M, Cubasch H, Joffe M, Laubscher R, et al. Adherence to cancer prevention recommendations is associated with a lower breast cancer risk in black urban South African women. Br J Nutr 2022;127:927-938.ArticlePubMed
- 16. Turati F, Dalmartello M, Bravi F, Serraino D, Augustin L, Giacosa A, et al. Adherence to the World Cancer Research Fund/American Institute for Cancer Research recommendations and the risk of breast cancer. Nutrients 2020;12:607.ArticlePubMedPMC
- 17. Oh JK, Han M, Kim B, Park EY. Adherence to cancer prevention guidelines and cancer incidence and mortality: a population-based cohort study. Cancer Res Treat 2023;55:15-27.ArticlePubMedPDF
- 18. Kim Y, Han BG; KoGES group. Cohort profile: the Korean Genome and Epidemiology Study (KoGES) consortium. Int J Epidemiol 2017;46:e20.ArticlePubMed
- 19. Health Examinees Study Group. The Health Examinees (HEXA) study: rationale, study design and baseline characteristics. Asian Pac J Cancer Prev 2015;16:1591-1597.ArticlePubMed
- 20. Shin S, Lee HW, Kim CE, Lim J, Lee JK, Kang D. Association between milk consumption and metabolic syndrome among Korean adults: results from the Health Examinees Study. Nutrients 2017;9:1102.ArticlePubMedPMC
- 21. Ahn Y, Kwon E, Shim JE, Park MK, Joo Y, Kimm K, et al. Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur J Clin Nutr 2007;61:1435-1441.ArticlePubMedPDF
- 22. Korean Nutrition Society. Food composition table. Recommended dietary allowances for Koreans. 7th ed. Seoul: Korean Nutrition Society; 2000. (Korean).
- 23. Shams-White MM, Brockton NT, Mitrou P, Romaguera D, Brown S, Bender A, et al. Operationalizing the 2018 World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) cancer prevention recommendations: a standardized scoring system. Nutrients 2019;11:1572.ArticlePubMedPMC
- 24. World Health Organization. Obesity: preventing and managing the global epidemic: report of a WHO consultation; 2000 [cited 2022 Sep 19]. Available from: https://apps.who.int/iris/handle/10665/42330.
- 25. Kim HJ, Lee YK, Koo H, Shin MJ. Dietary reference intakes of sodium for Koreans: focusing on a new DRI component for chronic disease risk reduction. Nutr Res Pract 2022;16(Suppl 1):S70-S88.ArticlePubMedPMCPDF
- 26. Kang MJ, Won YJ, Lee JJ, Jung KW, Kim HJ, Kong HJ, et al. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2019. Cancer Res Treat 2022;54:330-344.ArticlePubMedPMCPDF
- 27. Bogović Crnčić T, Ilić Tomaš M, Girotto N, Grbac Ivanković S. Risk factors for thyroid cancer: what do we know so far? Acta Clin Croat 2020;59(Suppl 1):66-72.PubMedPMC
- 28. El Kinany K, Huybrechts I, Kampman E, Boudouaya HA, Hatime Z, Mint Sidi Deoula M, et al. Concordance with the World Cancer Research Fund/American Institute for Cancer Research recommendations for cancer prevention and colorectal cancer risk in Morocco: a large, population-based case-control study. Int J Cancer 2019;145:1829-1837.ArticlePubMedPDF
- 29. Jones P, Cade JE, Evans CE, Hancock N, Greenwood DC. Does adherence to the World Cancer Research Fund/American Institute of Cancer Research cancer prevention guidelines reduce risk of colorectal cancer in the UK Women’s Cohort Study? Br J Nutr 2018;119:340-348.ArticlePubMed
- 30. Karavasiloglou N, Hüsing A, Masala G, van Gils CH, Turzanski Fortner R, Chang-Claude J, et al. Adherence to the World Cancer Research Fund/American Institute for Cancer Research cancer prevention recommendations and risk of in situ breast cancer in the European Prospective Investigation into Cancer and Nutrition (EPIC) cohort. BMC Med 2019;17:221.ArticlePubMedPMCPDF
- 31. Korn EL, Graubard BI, Midthune D. Time-to-event analysis of longitudinal follow-up of a survey: choice of the time-scale. Am J Epidemiol 1997;145:72-80.ArticlePubMed
- 32. Romaguera D, Vergnaud AC, Peeters PH, van Gils CH, Chan DS, Ferrari P, et al. Is concordance with World Cancer Research Fund/American Institute for Cancer Research guidelines for cancer prevention related to subsequent risk of cancer? Results from the EPIC study. Am J Clin Nutr 2012;96:150-163.ArticlePubMed
- 33. Korn AR, Reedy J, Brockton NT, Kahle LL, Mitrou P, ShamsWhite MM. The 2018 World Cancer Research Fund/American Institute for Cancer Research score and cancer risk: a longitudinal analysis in the NIH-AARP diet and health study. Cancer Epidemiol Biomarkers Prev 2022;31:1983-1992.ArticlePubMedPMCPDF
- 34. Avgerinos KI, Spyrou N, Mantzoros CS, Dalamaga M. Obesity and cancer risk: emerging biological mechanisms and perspectives. Metabolism 2019;92:121-135.ArticlePubMed
- 35. Ordóñez-Mena JM, Schöttker B, Mons U, Jenab M, Freisling H, Bueno-de-Mesquita B, et al. Quantification of the smoking-associated cancer risk with rate advancement periods: meta-analysis of individual participant data from cohorts of the CHANCES consortium. BMC Med 2016;14:62.PubMedPMC
- 36. International Agency for Research on Cancer. Schistosomes, liver flukes and Helicobacter pylori. Lyon: International Agency for Research on Cancer; 1994. p 1-241.
- 37. Shin A, Park S, Shin HR, Park EH, Park SK, Oh JK, et al. Population attributable fraction of infection-related cancers in Korea. Ann Oncol 2011;22:1435-1442.ArticlePubMed
- 38. Shin HR, Shin A, Jung KW, Park B, Choi KS, Kim Y, et al. Attributable cause of cancer in Korea in the year 2009. Goyang: National Cancer Center; 2015. p 221 (Korean).
- 39. Eom BW, Joo J, Kim S, Shin A, Yang HR, Park J, et al. Prediction model for gastric cancer incidence in Korean population. PLoS One 2015;10:e0132613.ArticlePubMedPMC
- 40. Schürmann R, Cronin M, Meyer JU. Estrogen plus progestin and colorectal cancer in postmenopausal women. N Engl J Med 2004;350:2417-2419.Article
- 41. Fernandez E, La Vecchia C, Balducci A, Chatenoud L, Franceschi S, Negri E. Oral contraceptives and colorectal cancer risk: a meta-analysis. Br J Cancer 2001;84:722-727.ArticlePubMedPMC
- 42. La Vecchia C, Franceschi S. Reproductive factors and colorectal cancer. Cancer Causes Control 1991;2:193-200.ArticlePubMedPDF
- 43. Wardle J, Haase AM, Steptoe A, Nillapun M, Jonwutiwes K, Bellisle F. Gender differences in food choice: the contribution of health beliefs and dieting. Ann Behav Med 2004;27:107-116.ArticlePubMed
- 44. Bärebring L, Palmqvist M, Winkvist A, Augustin H. Gender differences in perceived food healthiness and food avoidance in a Swedish population-based survey: a cross sectional study. Nutr J 2020;19:140.ArticlePubMedPMCPDF
- 45. He FJ, MacGregor GA. A comprehensive review on salt and health and current experience of worldwide salt reduction programmes. J Hum Hypertens 2009;23:363-384.ArticlePubMedPDF
- 46. Sharma AM, Arntz HR, Kribben A, Schattenfroh S, Distler A. Dietary sodium restriction: adverse effect on plasma lipids. Klin Wochenschr 1990;68:664-668.ArticlePubMedPDF
- 47. Ruppert M, Diehl J, Kolloch R, Overlack A, Kraft K, Göbel B, et al. Short-term dietary sodium restriction increases serum lipids and insulin in salt-sensitive and salt-resistant normotensive adults. Klin Wochenschr 1991;69 Suppl 25:51-57.PubMed
- 48. Kim J, Park S, Nam BH. Gastric cancer and salt preference: a population-based cohort study in Korea. Am J Clin Nutr 2010;91:1289-1293.ArticlePubMed
- 49. Shin JY, Kim J, Choi KS, Suh M, Park B, Jun JK. Relationship between salt preference and gastric cancer screening: an analysis of a nationwide survey in Korea. Cancer Res Treat 2016;48:1037-1044.ArticlePubMedPDF
- 50. Kang MJ, Won YJ, Lee JJ, Jung KW, Kim HJ, Kong HJ, et al. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2019. Cancer Res Treat 2022;54:330-344.ArticlePubMedPMCPDF
REFERENCES
Figure & Data
References
Citations
- Compliance with the WCRF/AICR Recommendations in Qualitative Adaptation and the Occurrence of Breast Cancer: A Case-Control Study
Beata Stasiewicz, Lidia Wadolowska, Maciej Biernacki, Malgorzata Anna Slowinska, Ewa Stachowska
Cancers.2024; 16(2): 468. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite


