Demographic characteristics and intravenous drug use among hepatitis C patients in the Kota Setar district, Kedah, Malaysia
Article information
Abstract
OBJECTIVES:
This study explored the demographic characteristics of hepatitis C patients in the Kota Setar (KS) district, Kedah, Malaysia, the prevalence of intravenous drug use (IVDU) as a risk factor among these patients, and the associations between IVDU and demographic characteristics.
METHODS:
Retrospective data pertaining to 713 patients from January 2009 to December 2013 were retrieved from hospital and disease notification records for analysis. The risk factors for hepatitis C virus (HCV) infection were grouped into IVDU and non-IVDU risk factors for analysis using multiple logistic regression.
RESULTS:
Of the hepatitis C patients included in this study, the most common age group was 31 to 40 years (30.2%), and male patients (91.2%) made up the overwhelming majority. Ethnic Malays constituted approximately 80.4% of the patients, and IVDU was the main risk factor (77.8%) for HCV infection. Multiple logistic regression showed that male patients were 59 times more likely to have IVDU as a risk factor for HCV infection. Single patients were 2.5 times more likely to have IVDU as a risk factor. Patients aged ≥71 years were much less likely than patients aged ≤30 years to have IVDU as a risk factor for HCV infection.
CONCLUSIONS:
IVDU was found to be an important risk factor for HCV infection among patients in the KS district. The factors associated with IVDU included age, sex, and marital status. Appropriate preventive measures should be developed to target the groups in which IVDU is most likely to be a risk factor for HCV infection.
INTRODUCTION
Hepatitis C is a major global health problem and a potential cause of substantial morbidity and mortality in the future. In 2013, the World Health Organization (WHO) estimated that approximately 150 million people, comprising approximately 3% of the world’s population, are chronically infected with hepatitis C virus (HCV). In addition, the WHO reported that more than 350,000 people die annually from hepatitis C-related liver disease [1]. The prevalence of HCV in Southeast Asia has been reported to be 2%, which is considered an intermediate level globally [2]. HCV can cause both acute and chronic liver disease, with eventual complications that include liver cirrhosis and hepatocellular carcinoma.
HCV is a small (55 nm to 65 nm), enveloped, positive-sense single-stranded RNA virus of the family Flaviviridae, and was first identified in 1989 [3]. Six basic genotypes exist, with multiple subtypes within each genotype [4,5]. HCV is most frequently spread through direct contact with infectious blood. In frequently, it may also be transmitted through sexual intercourse with an infected person or sharing personal items contaminated with HCV [1]. Risk factors include transfusion of blood and blood products, transplantation of solid organs from infected donors, intravenous drug use (IVDU), hemodialysis, occupational exposure to infected blood, tattooing, birth to an infected mother, and sexual intercourse with an infected partner [1,6].
A study conducted in Kuala Lumpur Hospital involving 119 HCV-infected patients from 1990 to 2000 found that the majority of patients (48.7%) were infected via blood transfusions [7]. The introduction of routine blood screening in 1991 has led to effective control of this infection route. However, patients who are already infected are at risk of developing advanced liver disease, contributing to a continuing rise in HCV-related morbidity and mortality that has been predicted by mathematical models [8-10]. Approximately 60% to 70% of chronically infected patients will eventually develop chronic liver disease; 5% to 20% will develop cirrhosis of the liver, and 1% to 5% will die of cirrhosis or hepatocellular carcinoma [1,6].
Relatively few publications have dealt with the epidemiological aspects of HCV infection in Malaysia. The studies that have been published were conducted on selected population subgroups, such as blood donors, intravenous drug users, and hemodialysis patients, ranging from 1993 to 2009 [11-13]. This study was motivated by the lack of local data, and focused primarily on the demographic data, risk factors, and complications of HCV patients in the Kota Setar (KS) district, Kedah, Malaysia. We aimed to study the demographic characteristics of hepatitis C patients, and to explore the associations of demographic characteristics and IVDU with HCV infection.
MATERIALS AND METHODS
A cross-sectional study involving patients in the KS district, Kedah, Malaysia was conducted from June 2013 to June 2014. The secondary data of all patients diagnosed with hepatitis C from January 2009 until December 2013 were included in this study. The enrollment criterion was the presence of antibodies to HCV as indicated by a positive screening test and confirmed by an enzyme-linked immunosorbenct assay (ELISA) kit, regardless of whether the infection was acute or chronic. The ELISA kit was AxSYM anti-HCV, a third-generation ELISA test (Abbott Diagnostics, Lake Forest, IL, USA).
All of the 713 HCV-infected patients were diagnosed via apositive anti-HCV screening test that was confirmed by ELISA. The secondary data gathered included demographic characteristics, risk factors, and data pertaining to clinical care. A data collection sheet was used to gather data from computerized medical records, notification forms, and hand-written case notes without including any identifiable information. A patient could have one or more risk factors. This study was registered with the Malaysian National Medical Research Register and approved by the Malaysian Medical Research Ethics Committee.
Our main goal was to explore associations between the demographic characteristics of hepatitis C patients and IVDU. Statistical analyses were performed using SPSS version 20.0 (IBM Corp., Armonk, NY, USA). Simple logistic regression was utilized to explore associations between demographic characteristics and IVDU. A p-value <0.05 was considered to indicate statistical significance [14].
RESULTS
Demographic characteristics
In the five-year period of the study, 713 patients were diagnosed with hepatitis C in the KS district, Kedah, Malaysia. The plurality of our patients (30.2%) were 31 to 40 years of age, followed by the age groups of 41 to 50 years (29.7%) and 51 to 60 years (19.6%). The overwhelming majority (91.2%) of the patients were male. According to ethnicity, 80.4% of patients were Malay, and the next most prevalent ethnic groups were Chinese (14.2%) and Indian (5.0%). With regard to marital and employment status, pluralities of the patients were currently married (37.9%) and unemployed (33.5%) (Table 1).
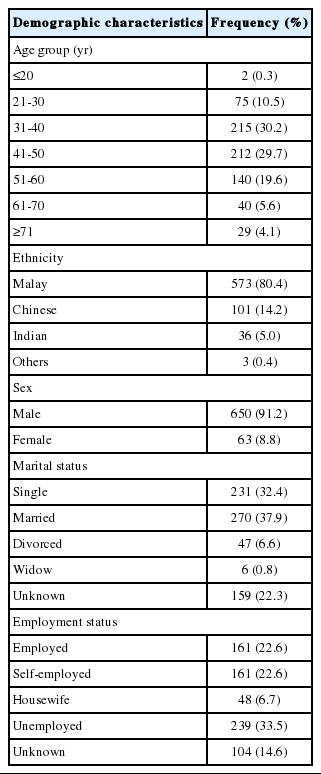
Demographic characteristics of patients diagnosed with hepatitis C in the Kota Setar district, Kedah, Malaysia from 2009 to 2013
Intravenous drug use vs. non-intravenous drug use risk factors
We categorized the risk factors as IVDU and non-IVDU risk factors. In general, IVDU (77.8%) was the most prominent risk factor among our patients. The other risk factors were blood/blood product transfusion (4.9%), sexual contact with an infected person (3.9%), and hemodialysis (3.5%) (Table 2).
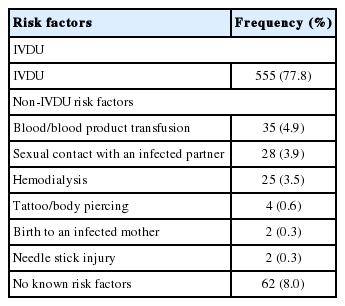
Risk factors among patients diagnosed with hepatitis C in the Kota Setar district, Kedah, Malaysia from 2009 to 2013
Complications of hepatitis C
The complications identified in this study were decompensated liver disease (8.4%), cirrhosis of the liver (3.9%), and hepatocellular carcinoma (3.4%).
The main methods of diagnosing liver cirrhosis are abdominal ultrasonography and liver biopsy if the diagnosis is uncertain [15]. Hepatic decompensation is defined by the development of jaundice, ascites, variceal bleeding, or hepatic encephalopathy. Its diagnosis is guided by the Child-Pugh classification of liver disease. Hepatocellular carcinoma is diagnosed according to the following guidelines [16,17]:
a) A focal lesion in the liver of a patient with cirrhosis,
b) Assessment by spiral computed tomography of the liver or magnetic resonance imaging with contrast enhancement,
c) Liver biopsy is rarely required in circumstances in which the diagnosis of hepatocellular carcinoma is certain after clinical, laboratory, and radiographic evaluation.
However, the majority (84.3%) of our patients had no known complications during the study period. This could have been due to limitations in our data regarding the outcomes of HCV infection (Table 3).
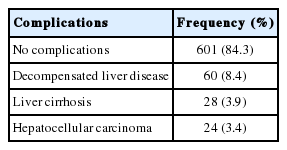
Complications of hepatitis C infection in the Kota Setar district, Kedah, Malaysia from 2009 to 2013
Demographic characteristics and intravenous drug use
Further inferential analysis was performed using logistic regression between demographic characteristics and IVDU. In a simple logistic regression analysis, age group, sex, marital status, and ethnicity were found to be associated with IVDU as a risk factor for HCV. After adjusting for every variable using multiple logistic regression, age group, sex, and marital status remained significantly associated with IVDU as a risk factor for HCV.
In particular, men were 59 times more likely to have IVDU as a risk factor for HCV infection. Another notable finding was that unmarried patients were 2.5 times more likely to have IVDU as a risk factor. Patients aged ≥71 years old were much less likely than those ≤30 years of age to have IVDU as a risk factor for HCV infection (Table 4).

Association between demographic characteristics and intravenous drug use as a risk factor for hepatitis C
DISCUSSION
HCV is most effectively transmitted via large or repeated direct percutaneous exposure to infected blood [18]. In this study, the most important risk factor for HCV infection was IVDU. This finding corresponds to those of many other studies, such as one that found that the risk of HCV infection was three times as high among subjects who had used marijuana 100 times or more (adjusted odds ratio [OR], 2.99; 95% confidence interval [CI], 1.69 to 5.27) [19]. Moreover, subjects who had ever used cocaine were found to be almost five times as likely to be infected with HCV (95% CI, 2.49 to 8.87) [19]. The above findings have established a strong link between drug use and HCV infection. Globally, the illegal injection of drugs has been established as the predominant mode of transmission of HCV [18]. From 1999 to 2002, intravenous drug users had a markedly higher prevalence of HCV infection (57.5%) than people with no history of drug use (0.7%) in the US [20]. Garfein et al. [21] likewise found that young adults in the US who were intravenous drug users had a higher risk of becoming infected with HCV [21]. In addition, HCV seroprevalence was found to be independently related to reusing syringes at least once in the past six months (OR, 3.81; 95% CI, 1.39 to 11.00) and injecting cocaine (OR, 4.29; 95% CI, 1.53 to 12.01) [21].
In the current study, we determined that age was significantly associated with IVDU among HCV-infected patients. The top three age groups among our sample of hepatitis C patients were 31 to 40 years, 41 to 50 years, and 51 to 60 years. In contrast, in a study of Malaysian blood donors, HCV infection was most common in subjects more than 40 years old [13]. A review in Brazil found that the prevalence of HCV infection was high among individuals over 30 years old, with a peak in patients aged 50 to 59 years (3.8%) [22]. In that study, the most important risk factors included intravenous drug use, although their study contained relatively little information on the distribution of risk factors. The fact that these studies reported similar findings about which age groups are most affected by HCV infection suggests that the risk of being infected by HCV is highest in people at least 30 years of age for whom IVDU is an important risk factor. Globally, Alter et al. [18] found that the age-specific prevalence of HCV infection increased steadily with age in Turkey, Spain, Italy, Japan, and China, and that patients more than 50 years old accounted for most of the burden of HCV infection [18]. The prevalence of HCV infection in Egypt was also found to increase with age, although a high rate of infection was observed in all age groups [18]. It was hypothesized that a greater risk of infection existed in the past, roughly 40 to 60 years previously [22].
The current study found that men made up the overwhelming majority of HCV cases (91.2%), and male HCV patients were found to be 59 times more likely to have a history of IVDU. Our findings complement those of a study in Iran in which the prevalence of HCV infection among male inmates was found to be 93.0%, and IVDU was the top risk factor [23]. Another study in Kuala Lumpur likewise showed a preponderance of male patients (74.0%) among all HCV cases, irrespective of their ethnicity, although the main risk factor in that study was a history of blood transfusions [7]. The differences between the findings of that study and those of the current study may be due to the fact that the former study was conducted almost 15 years ago, when the main transmission route of HCV was blood transfusions. In Vancouver, female adolescents were found to have a higher rate of HCV seroconversion, and a gender-stratified analysis revealed the presence of similar risk factors, such as the injection of heroin and crystal methamphetamine, in both genders [24]. The difference between the findings of that study and those of the current study could be accounted for by the presence of sharp differences in the study populations and the social and cultural contexts. Another study in the US likewise found no significant difference between genders in the prevalence of sharing needles during drug use [25].
This study found that the subjects who were single were 2.5 times more likely to have been exposed to HCV through IVDU than those who were married. Limited information exists from previous studies that would help contextualize this finding. One of the most valuable studies in this regard was conducted in the US, and it was found that unmarried people comprised more than half of the subjects with all durations of intravenous drug use [21]. As mentioned above, HCV infection may lead to complications, meaning that the prevention of HCV transmission should be emphasized in order to reduce its morbidity and mortality. Primary prevention is especially crucial in reducing the disease burden posed by HCV infection. Risk reduction counseling and services should also be made widely available in the community [26]. Moreover, the elimination of intravenous drug abuse would certainly reduce the transmission of HCV infection. An excellent example is the use of methadone, which eliminates intravenous injections and thereby addresses the main risk factor identified in this study.
The main strength of this study is that it was conducted in a multiethnic setting and included an entire district in the state of Kedah. Moreover, the district analyzed in the study is one of the most heavily populated districts in the state, with a mixture of urban and suburban settings. Thus, these results can be applied to urban and suburban populations. To our knowledge, this is the first study on this topic conducted in Kedah, Malaysia, and this study was motivated by the scarcity of information on HCV infection in this region. One limitation of this study is the fact that comprehensive data were not always available; for instance, only incomplete data about the complications of HCV infections were available and most of the patients are still under follow up as complications may take a long time to develop. Another limitation was that tests for HCV RNA were not performed among our patients, meaning that we could not identify patients who had cleared an HCV infection in the past or who had false positive reactions to the tests measuring HCV antibodies. This study indirectly underscores the need for widely implementing programs designed to facilitate the early detection of HCV infections. Early testing should be offered to those at high risk of HCV infection, such as intravenous drug users [26]. After a case of HCV infection is detected, appropriate medical management, counseling, and follow-up are warranted in order to contain the spread of disease in a high--risk population. This step would likely be the cornerstone of controlling the transmission of HCV infection in the community. Moreover, early and appropriate treatment for HCV is curative.
In conclusion, IVDU was found to be a major risk factor for HCV infection in the KS district, Kedah, Malaysia. Age, male gender, and single status were strongly associated with IVDU as a risk factor for HCV infection. As a result, preventive measures targeting high-risk groups should be developed in order to control HCV infection and to reduce its burden of morbidity and mortality in the coming years.
Notes
The authors have no conflicts of interest to declare for this study.