National Infectious Diseases Surveillance data of South Korea
Article information
Abstract
The Korea Centers for Disease Control and Prevention (KCDC) operate infectious disease surveillance systems to monitor national disease incidence. Since 1954, Korea has collected data on various infectious diseases in accordance with the Infectious Disease Control and Prevention Act. All physicians (including those working in Oriental medicine) who diagnose a patient with an infectious disease or conduct a postmortem examination of an infectious disease case are obliged to report the disease to the system. These reported data are incorporated into the database of the National Infectious Disease Surveillance System, which has been providing web-based real-time surveillance data on infectious diseases since 2001. In addition, the KCDC analyzes reported data and publishes the Infectious Disease Surveillance Yearbook annually.
INTRODUCTION
In general, national notifiable infectious diseases are those that cause severe infections with poor prognoses; are highly contagious and can be prevented with appropriate quarantine, vaccination, or chemical therapy; or require management and control by conducting research. The designation of a notifiable disease is multi factorial. As a result, there are numerous discrepancies in the definition of these diseases across various countries. The incidence of infectious diseases and issues related to these diseases change with time; therefore, frequent updates to relevant information are required. The purpose of designating national notifiable infectious diseases is to protect the public from the threat of infectious diseases by effectively controlling the disease using an accurate and sensitive surveillance system and by appropriately allocating the available resources.
The incidence of national notifiable infectious diseases is calculated using data reported by medical providers (Western and Oriental medical doctors) to health institutions in accordance with the Infectious Disease Control and Prevention Act [1]. Physicians working at clinics or hospitals report cases of infectious disease to their regional health center. These data are reviewed by local health authorities and transferred to the Korea Centers for Disease Control and Prevention (KCDC). After final confirmation from the KCDC, a report of these national statistics is published. According to the diagnosis and reporting standards in the “case definitions for national notifiable infectious diseases [2],” cases with an infectious disease are classified as three groups; an infectious disease patient (pathogen identifier), a patient with a suspected infection (unidentified pathogen carrier), or a pathogen carrier. The scope of each infectious disease report varies depending on the disease characteristics.
The Mandatory Surveillance System requires obligatory reporting on infectious diseases ‘without delay’ to a district health center. In comparison, the Sentinel Surveillance System receives the report on weekly from the designated sites. In addition, the Complementary Sentinel Surveillance System consists of a school-based infectious disease surveillance program and ocular infectious disease surveillance program.
Since the start of the surveillance system, many changes to the computer system structure have made. In the early stages of the construction of the surveillance system, a client-server based method between health institutions was the main way of data collection. However, from January 18, 2007, the reporting method using paper-based assessment was converted to a computer-based assessment. This computerized disease surveillance system was more efficient, flexible, and convenient than the paper-based assessment. In 2009, an internet-based reporting system was developed for use in clinics and hospitals. This system allowed for near real-time assessments the incidence of infectious diseases nationwide as well as quick data collection and a rapid response. From May 18, 2007, a web statistics system on infectious disease (http://stat.cdc.go.kr) was established. These efforts improved public accessibility to system data. In 2011, this website was updated as the infectious disease web-statistics system (http://is.cdc.go.kr/nstat/index.jsp) and it provides data on 54 infectious diseases that are mandatorily reported. In addition, the Infectious Disease Surveillance Yearbook, which organizes and analyzes the overall incidence of national notifiable infectious diseases, is published and distributed annually [3]. Reported infectious disease surveillance data since 1954 which is based on the Infectious Disease Control and Prevention Act is presented in Table 1.
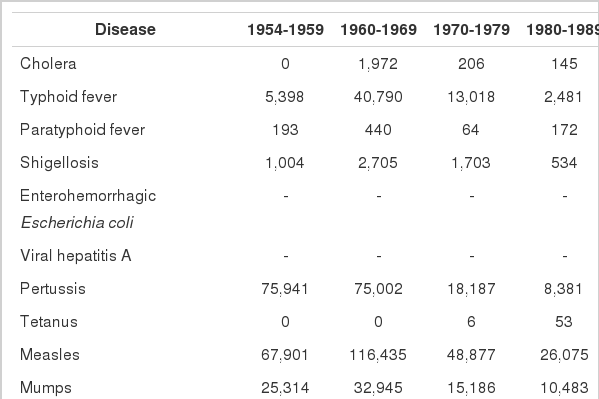
Reported cases of national infectious diseases in South Korea, 1954-2013
DATA ACCESSIBILITY
The Disease Web Statistics System (http://is.cdc.go.kr/nstat/index.jsp) provides real-time data on 54 national notifiable infectious diseases specified by area, sex, age, infected region, and period. Moreover, it is possible to compare the current weekly incidence to that of the previous year. These data can be presented as tables or figures, and downloaded as a spreadsheet.
KEY FINDINGS AND PUBLICATIONS
The Sentinel Surveillance System monitors 24 of the 78 national notifiable infectious diseases. The KCDC uses these data to estimate the trends and patterns of some infectious diseases. The data only consists of the number of reported cases at each sentinel site and does not contain detailed information of each individual case; therefore, the national incidence of sentinel infectious diseases is difficult to estimate using the sentinel surveillance data. The main purpose of this data is to determine trends and patterns of infectious diseases.
For example, one study used these sentinel surveillance data to analyze influenza cases and hospitalizations of severe pneumonia nationwide [4]. This analysis used the sentinel surveillance data on sentinel influenza sites from 2005 to 2010 as well as national health insurance claims data from the Health Insurance Review and Assessment Service (influenza diagnostic codes J09-J11). In addition, the number of influenza patients per month, the total numbers of out-patients, and the total numbers of hospital visits were extracted for analysis. With these data, an estimation model was created (Figure 1) [4].
Procedure of model development to calculate influenza incidence. KCDC, Korea Centers for Disease Control and Prevention; a is constant, B1, B2, B3, C1, C2, and C3 are coefficients from this regression model.
From Roh YK. Modeling the national pandemic influenza cases and inpatients of pneumonia in Korea. Osong: Korea Centers for Disease Control and Prevention; 2011 [4].
In this paper, the number of influenza patients in Seoul on November 2009 was estimated using this formula; final number of patients=constant + C1×(estimated number of patients ×W3)+C2×(year-2004). Minor differences between the estimated value based on the model and the health insurance claims data were found.
STRENGTHS AND WEAKNESSES
The reporting of national notifiable diseases is standardized and provides up-to-date information including diagnostics and the epidemiological characteristics of each infectious disease. Moreover, these data are distributed to healthcare sites regularly. However, the reporting of national notifiable infectious diseases in South Korea relies on the passive reporting of healthcare workers. Thus, the reporting rate is relatively low. Nevertheless, the number of patients with an infectious disease can be estimated using existing data. The KCDC not only seeks to encourage the reporting of infectious diseases that present at healthcare sites but also continues to develop ways to improve the current systems using multidimensional approaches, not limited to passive reporting.
Notes
The authors have no conflicts of interest to declare for this study.
SUPPLEMENTARY MATERIAL
Supplementary material is available at http://www.e-epih.org/.