
Articles
- Page Path
- HOME > Epidemiol Health > Volume 43; 2021 > Article
-
COVID-19: Original Article
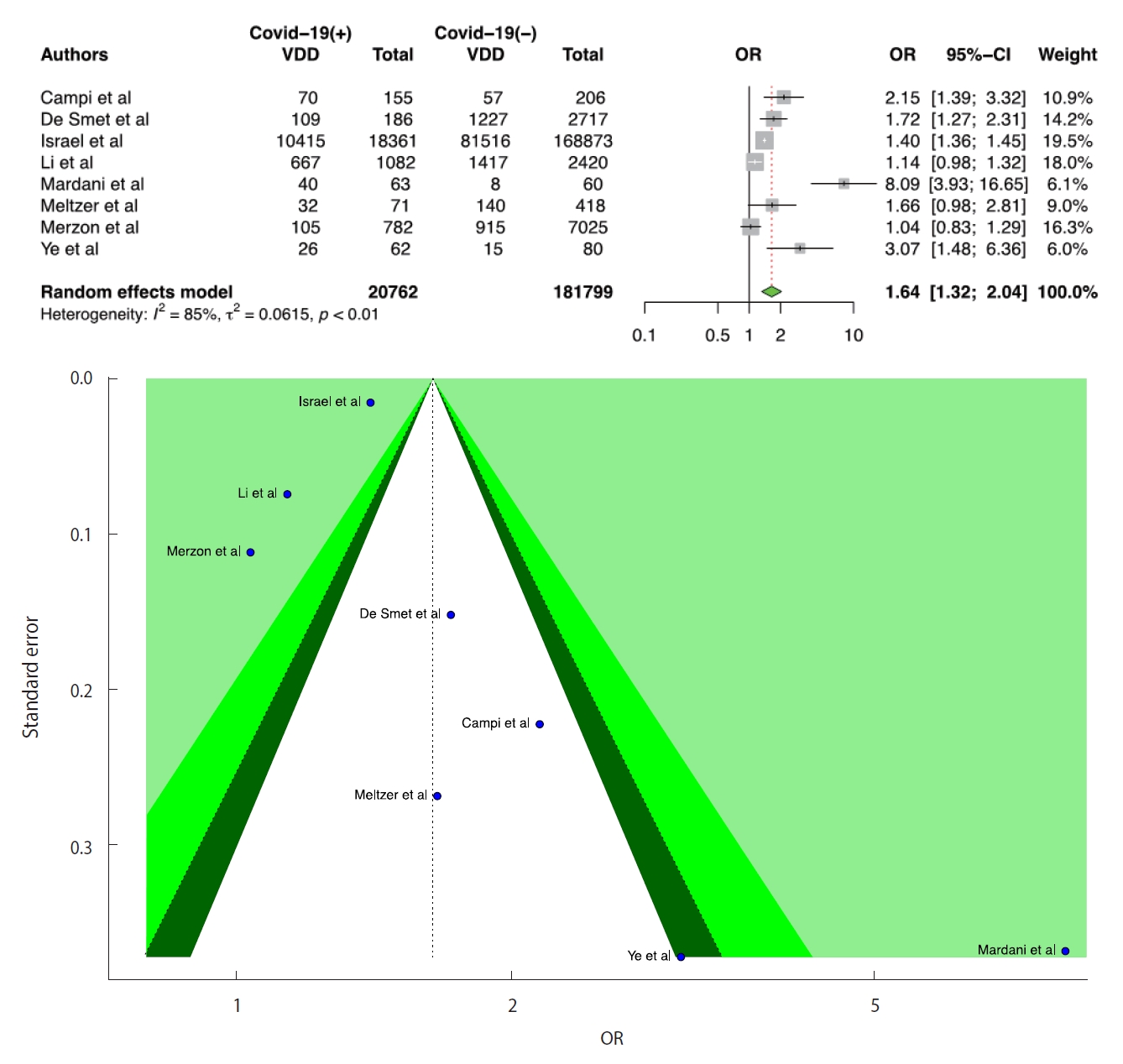
The role of vitamin D deficiency on COVID-19: a systematic review and meta-analysis of observational studies -
Mehmet Onur Kaya1
 , Esra Pamukçu2, Burkay Yakar3
, Esra Pamukçu2, Burkay Yakar3 -
Epidemiol Health 2021;43:e2021074.
DOI: https://doi.org/10.4178/epih.e2021074
Published online: September 23, 2021
1Department of Biostatistics and Medical Informatics, Firat University School of Medicine, Elazığ, Turkey
2Department of Statistics, Faculty of Science, Fırat University, Elazığ, Turkey
3Department of Family Medicine, Firat University School of Medicine, Elazığ, Turkey
- Correspondence: Esra Pamukçu Department of Statistics, Faculty of Science, Fırat University, Elazığ 23119, Turkey E-mail: epamukcu@firat.edu.tr
• Received: July 27, 2021 • Accepted: September 23, 2021
©2021, Korean Society of Epidemiology
This is an open-access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

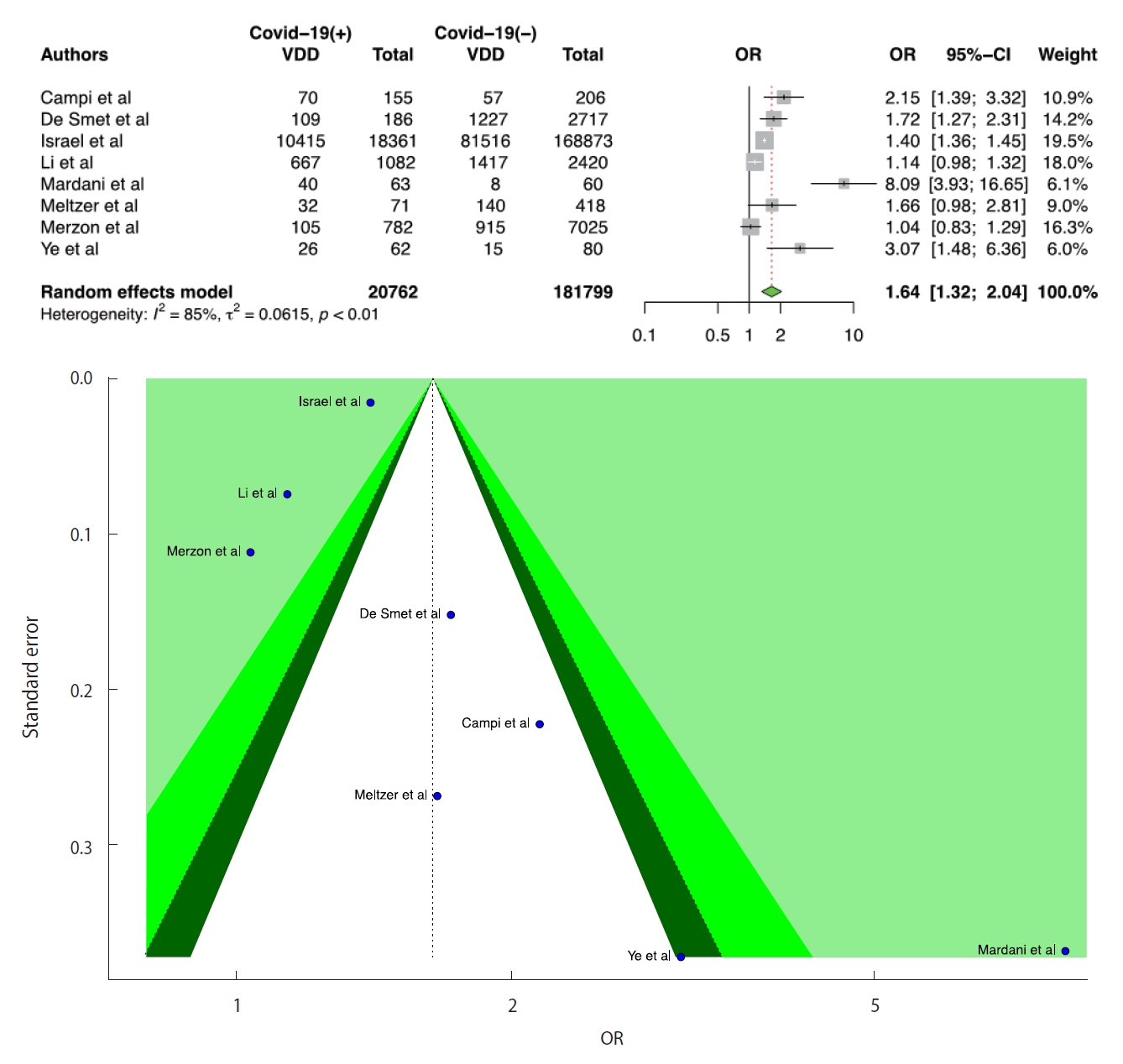
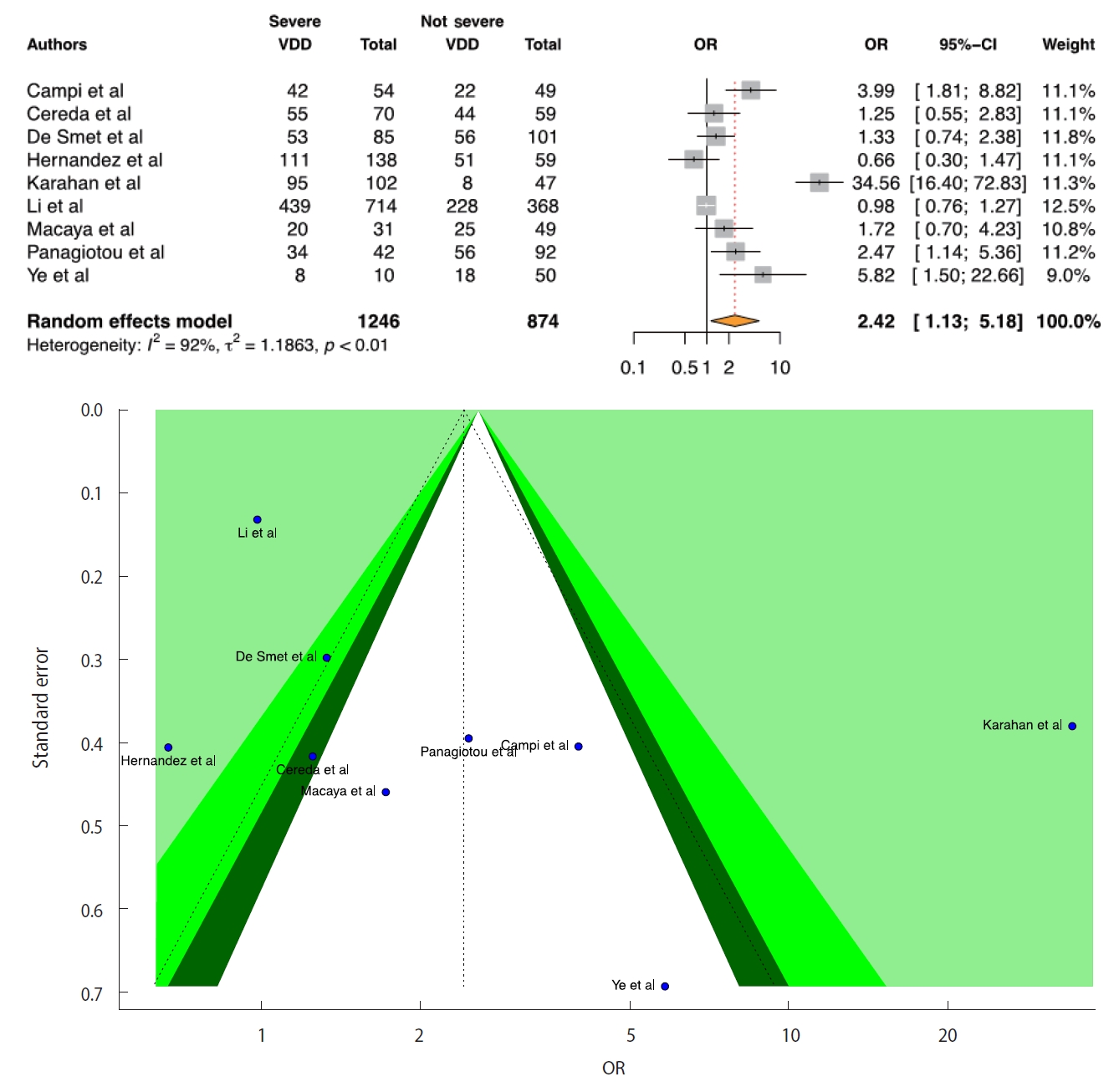
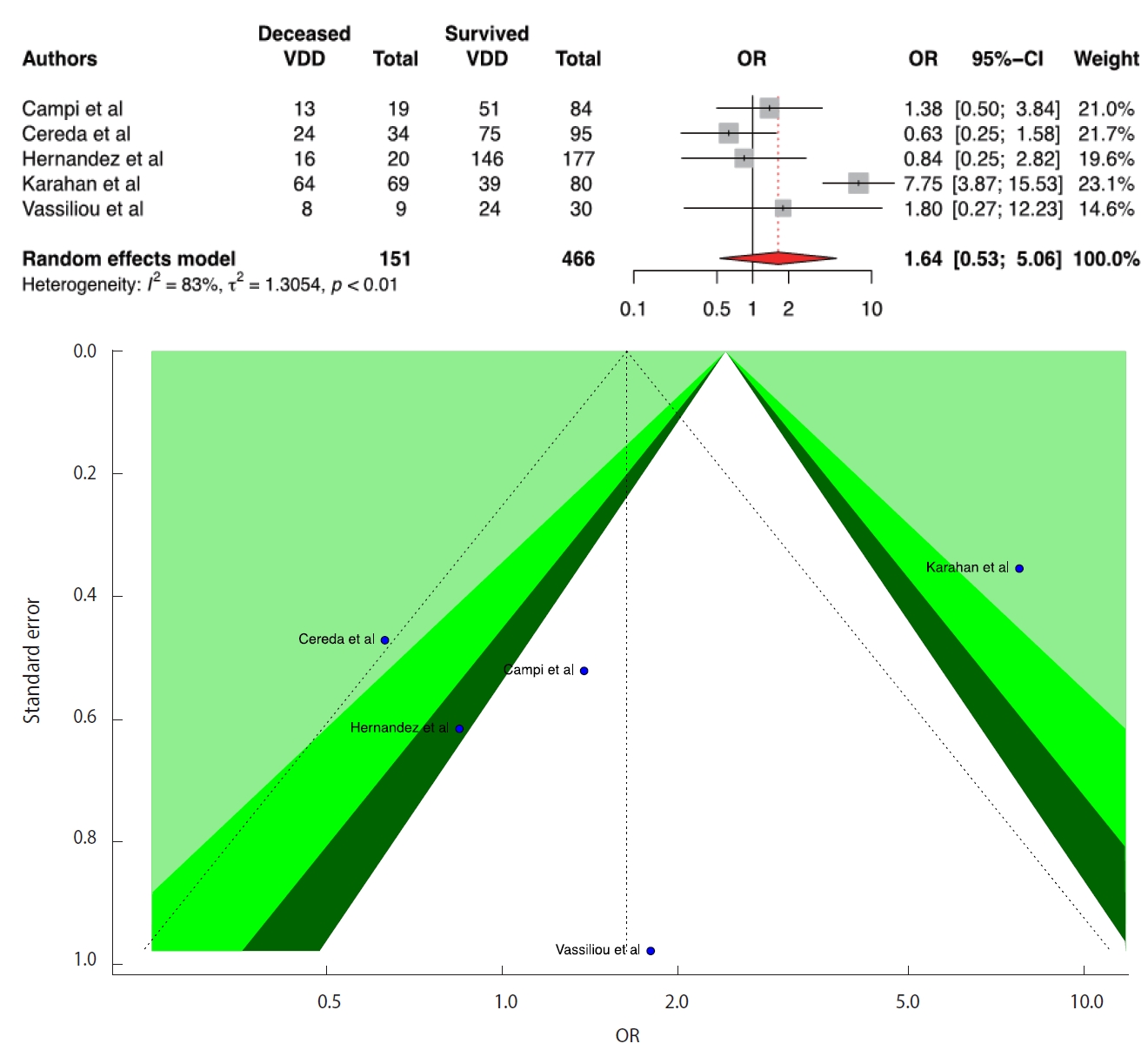
Figure & Data
References
Citations
Citations to this article as recorded by 
- 25-Hydroxyvitamin D concentrations do not affect the humoral or cellular immune response following SARS-CoV-2 mRNA vaccinations
A.H.A. Lavell, A.E. Schramade, J.J. Sikkens, K. van der Straten, K.A. van Dort, M.A. Slim, B. Appelman, L.A. van Vught, A.P.J. Vlaar, N.A. Kootstra, M.J. van Gils, Y.M. Smulders, R.T. de Jongh, M.K. Bomers, Brent Appelman, Diederik Beek van de, Marije K.
Vaccine.2024; 42(7): 1478. CrossRef - The Protective Effect of Serum Levels of Vitamins C, D, and E and IgG and IgM Antibodies in Individuals Vaccinated Against COVID-19 and Experienced Disease Relapse
Ashkan Alamdary, Alireaza Gholami, Maryam Shahali, Delaram Doroud, Rasul Moukhah, Mohammad Javad Hossein Tehrani, Rajab Mardani, Nayebali Ahmadi
Jundishapur Journal of Microbiology.2024;[Epub] CrossRef - Exploring demographical, clinical, and dietary determinants of vitamin D deficiency among adults in Douala, Cameroon during the COVID-19 era
Arlette Flore Moguem Soubgui, Wilfried Steve Ndeme Mboussi, Loick Pradel Kojom Foko, Elisée Libert Embolo Enyegue, Martin Luther Koanga Mogtomo
Heliyon.2024; 10(3): e24926. CrossRef - Dynamic Shifts in Vitamin D Status Following Liposuction: Implications for Patient Monitoring and Health
Hüseyin KANDULU
Ağrı Tıp Fakültesi Dergisi.2024; 2(1): 1. CrossRef - Vitamin D in the prevention or treatment of COVID-19
Adrian R. Martineau
Proceedings of the Nutrition Society.2023; 82(2): 200. CrossRef - 100 years of vitamin D. The impact of vitamin D level in the time of COVID-19 pandemic
K. A. Golovatyuk, A. A. Mikhailova, D. I. Lagutina, A. T. Chernikova, T. L. Karonova
Russian Journal for Personalized Medicine.2023; 2(6): 33. CrossRef - Vitamin D3 and COVID-19 Outcomes: An Umbrella Review of Systematic Reviews and Meta-Analyses
Fausto Petrelli, Simone Oldani, Karen Borgonovo, Mary Cabiddu, Giuseppina Dognini, Mara Ghilardi, Maria Chiara Parati, Daniela Petro’, Lorenzo Dottorini, Carmen Rea, Veronica Lonati, Andrea Luciani, Antonio Ghidini
Antioxidants.2023; 12(2): 247. CrossRef - Genetic Variations of the Vitamin D Metabolic Pathway and COVID-19 Susceptibility and Severity: Current Understanding and Existing Evidence
Nipith Charoenngam, Aunchalee Jaroenlapnopparat, Sofia K. Mettler, Ashna Grover
Biomedicines.2023; 11(2): 400. CrossRef - MC-Au/MSS-Z8 porous network assisted advanced electrochemical immunosensing of 25-hydroxyvitamin D3
Amandeep Kaur, Lavisha, Ganga Ram Chaudhary, Nirmal Prabhakar
Talanta.2023; 257: 124376. CrossRef - Nutritional deficiencies that may predispose to long COVID
John V. Schloss
Inflammopharmacology.2023; 31(2): 573. CrossRef - Changes in Food Consumption Trends among American Adults since the COVID-19 Pandemic
Lillie Monroe-Lord, Elgloria Harrison, Azam Ardakani, Xuejling Duan, Lily Spechler, Tia D. Jeffery, Phronie Jackson
Nutrients.2023; 15(7): 1769. CrossRef - The Role of Diet and Specific Nutrients during the COVID-19 Pandemic: What Have We Learned over the Last Three Years?
Petra Rust, Cem Ekmekcioglu
International Journal of Environmental Research and Public Health.2023; 20(7): 5400. CrossRef - The role of serum vitamin 25(OH)D concentration in the Covid-19 pandemic in children
Chrysoula Kosmeri, Foteini Balomenou, Dimitrios Rallis, Maria Baltogianni, Vasileios Giapros
British Journal of Nutrition.2023; 130(3): 417. CrossRef - Vitamin D metabolism parameters in hospitalized COVID-19 patients
A. A. Mikhailova, K. A. Golovatyuk, D. I. Lagutina, A. T. Chernikova, E. Yu. Vasilieva, E. S. Bykova, T. L. Karonova
Translational Medicine.2023; 10(2): 69. CrossRef - Characteristics, comorbidities and laboratory measures associated with disease severity and poor prognosis in young and elderly patients with COVID-19 admitted to medical wards in Emilia-Romagna region, Italy: a multicentre retrospective study
Sirio Fiorino, Andrea Carusi, Alessandro Zappi, Fabio Tateo, Luca Peruzzo, Melissa Zanardi, Francesco Savelli, Giulia Di Marzio, Silvia Cesaretti, Francesca Dazzani, Raffaella Francesconi , Paolo Leandri , Gianfranco Tortorici , Susanna Vicari , Dora Melu
Italian Journal of Medicine.2023;[Epub] CrossRef - Six years’ experience and trends of serum 25-hydroxy vitamin D concentration and the effect of vitamin D3 consumption on these trends
László Horváth, Sara Mirani, Michael Magdy Fahmy Girgis, Szilvia Rácz, Ildikó Bácskay, Harjit Pal Bhattoa, Béla E. Tóth
Frontiers in Pharmacology.2023;[Epub] CrossRef - Neuroimmunological Effect of Vitamin D on Neuropsychiatric Long COVID Syndrome: A Review
Ting-Bin Chen, Ching-Mao Chang, Cheng-Chia Yang, I-Ju Tsai, Cheng-Yu Wei, Hao-Wen Yang, Chun-Pai Yang
Nutrients.2023; 15(17): 3802. CrossRef - The effect of vitamin D deficiency on the cellular immunity of patients in the early stage of COVID-19 disease
Ali Sadeg, Abbas Arrak
Bionatura.2023; 8(CSS 3): 1. CrossRef - Distribution of Vitamin D Status in a Group from Syrian Society
Talleh Almelli
Jordan Journal of Pharmaceutical Sciences.2023; 16(4): 680. CrossRef - Effects of environmental parameters and their interactions on the spreading of SARS-CoV-2 in North Italy under different social restrictions. A new approach based on multivariate analysis
Fabio Tateo, Sirio Fiorino, Luca Peruzzo, Maddalena Zippi, Dario De Biase, Federico Lari, Dora Melucci
Environmental Research.2022; 210: 112921. CrossRef - The Relation between Vitamin D Level and Lung Clearance Index in Cystic Fibrosis—A Pilot Study
Mihaela Dediu, Ioana Mihaiela Ciuca, Liviu Laurentiu Pop, Daniela Iacob
Children.2022; 9(3): 329. CrossRef - Effect of Cholecalciferol Supplementation on the Clinical Features and Inflammatory Markers in Hospitalized COVID-19 Patients: A Randomized, Open-Label, Single-Center Study
Tatiana L. Karonova, Ksenia A. Golovatyuk, Igor V. Kudryavtsev, Alena T. Chernikova, Arina A. Mikhaylova, Arthur D. Aquino, Daria I. Lagutina, Ekaterina K. Zaikova, Olga V. Kalinina, Alexey S. Golovkin, William B. Grant, Evgeny V. Shlyakhto
Nutrients.2022; 14(13): 2602. CrossRef - Vitamin D Endocrine System and COVID-19: Treatment with Calcifediol
Jose Manuel Quesada-Gomez, José Lopez-Miranda, Marta Entrenas-Castillo, Antonio Casado-Díaz, Xavier Nogues y Solans, José Luis Mansur, Roger Bouillon
Nutrients.2022; 14(13): 2716. CrossRef - Impaired Vitamin D Metabolism in Hospitalized COVID-19 Patients
Alexandra Povaliaeva, Viktor Bogdanov, Ekaterina Pigarova, Larisa Dzeranova, Nino Katamadze, Natalya Malysheva, Vitaliy Ioutsi, Larisa Nikankina, Liudmila Rozhinskaya, Natalia Mokrysheva
Pharmaceuticals.2022; 15(8): 906. CrossRef - Vitamin D and COVID-19. Two years of research
Andrey P. Fisenko, Svetlana G. Makarova, Dmitry S. Yasakov, Irina Yu. Pronina, Oksana A. Ereshko, Irina G. Gordeeva, Albina A. Galimova, Tamara R. Chumbadze, Evgeny Е. Emelyashenkov, Ayina M. Lebedeva
Russian Pediatric Journal.2022; 25(3): 199. CrossRef - Vitamin D as the essential immunonutrient – the evidence base update: A review
Svetlana G. Makarova, Evgeny E. Emelyashenkov, Dmitry S. Yasakov, Irina Yu. Pronina, Oksana A. Ereshko, Irina G. Gordeeva, Albina A. Galimova, Tamara R. Chumbadze, Ayina M. Lebedeva
Pediatrics. Consilium Medicum.2022; (2): 133. CrossRef - COVID-19 Severity and Mortality in Two Pandemic Waves in Poland and Predictors of Poor Outcomes of SARS-CoV-2 Infection in Hospitalized Young Adults
Laura Ziuzia-Januszewska, Marcin Januszewski, Joanna Sosnowska-Nowak, Mariusz Janiszewski, Paweł Dobrzyński, Alicja A. Jakimiuk, Artur J. Jakimiuk
Viruses.2022; 14(8): 1700. CrossRef - Serum vitamin D levels and COVID-19 during pregnancy: A systematic review and meta-analysis
Sadegh Mazaheri-Tehrani, Mohammad Hossein Mirzapour, Maryam Yazdi, Mohammad Fakhrolmobasheri, Amir Parsa Abhari
Clinical Nutrition ESPEN.2022; 51: 120. CrossRef - Administration of vitamin D and its metabolites in critically ill adult patients: an updated systematic review with meta-analysis of randomized controlled trials
Johannes Menger, Zheng-Yii Lee, Quirin Notz, Julia Wallqvist, M. Shahnaz Hasan, Gunnar Elke, Martin Dworschak, Patrick Meybohm, Daren K. Heyland, Christian Stoppe
Critical Care.2022;[Epub] CrossRef - Prevention of covid-19 and other acute respiratory infections with cod liver oil supplementation, a low dose vitamin D supplement: quadruple blinded, randomised placebo controlled trial
Sonja H Brunvoll, Anders B Nygaard, Merete Ellingjord-Dale, Petter Holland, Mette Stausland Istre, Karl Trygve Kalleberg, Camilla L Søraas, Kirsten B Holven, Stine M Ulven, Anette Hjartåker, Trond Haider, Fridtjof Lund-Johansen, John Arne Dahl, Haakon E M
BMJ.2022; : e071245. CrossRef - Adipokines, and not vitamin D, associate with antibody immune responses following dual BNT162b2 vaccination within individuals younger than 60 years
Mariana Pavel-Tanasa, Daniela Constantinescu, Corina Maria Cianga, Ecaterina Anisie, Ana Irina Mereuta, Cristina Gabriela Tuchilus, Petru Cianga
Frontiers in Immunology.2022;[Epub] CrossRef - Vitamin D intoxication induced severe hypercalcemia from self-medication for COVID-19 infection: a public health problem?
Stefano PINI, Giuseppe SCAPARROTTA, Valentina DI VICO, Antonio FRAGASSO, Lucia F. STEFANELLI, Federico NALESSO, Lorenzo A. CALÒ
Minerva Endocrinology.2022;[Epub] CrossRef - Novel CYP11A1-Derived Vitamin D and Lumisterol Biometabolites for the Management of COVID-19
Shariq Qayyum, Radomir M. Slominski, Chander Raman, Andrzej T. Slominski
Nutrients.2022; 14(22): 4779. CrossRef - COVID-19 Prevention: Vitamin D Is Still a Valid Remedy
Rachel Nicoll, Michael Y. Henein
Journal of Clinical Medicine.2022; 11(22): 6818. CrossRef - Integrated bioinformatics and in silico approaches reveal the biological targets and molecular mechanisms of 1,25-dihydroxyvitamin D against COVID-19 and diabetes mellitus
Fanqiang Zeng, Yongli Xu, Chaoling Tang, Zhigang Yan, Chaohe Wei
Frontiers in Nutrition.2022;[Epub] CrossRef - Can vitamin D status influence seroconversion to SARS-COV2 vaccines?
Endrit Shahini, Francesco Pesce, Antonella Argentiero, Antonio Giovanni Solimando
Frontiers in Immunology.2022;[Epub] CrossRef - Cholecalciferol as part of complex therapy for acute COVID-19
K.A. Golovatyuk, T.L. Karonova, A.A. Mikhailova, D.I. Lagutina, A.T. Chernikova, E.Yu. Vasilieva, E.V. Shlyakhto
Profilakticheskaya meditsina.2022; 25(12): 106. CrossRef - Vitamin D Metabolism Gene Polymorphisms and Their Associated Disorders: A
Literature Review
Mohamed Abouzid, Franciszek Główka, Leonid Kagan, Marta Karaźniewicz-Łada
Current Drug Metabolism.2022; 23(8): 630. CrossRef - Nutraceuticals in prevention and management of COVID-19
Ivana Đuričić, Milica Zrnić-Ćirić, Bojana Vidović, Vanja Todorović, Nevena Dabetić, Nevena Ivanović
Hrana i ishrana.2021; 62(2): 7. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite- Figure
-


- Related articles
-
- Dietary intake and cancer incidence in Korean adults: a systematic review and meta-analysis of observational studies
- Associations of daily diet-related greenhouse gas emissions with the incidence and mortality of chronic diseases: a systematic review and meta-analysis of epidemiological studies
- The prevalence of Q fever in the Eastern Mediterranean region: a systematic review and meta-analysis
- The relationship between metabolic syndrome and its components with bladder cancer: a systematic review and meta-analysis of cohort studies

