Articles
- Page Path
- HOME > Epidemiol Health > Volume 45; 2023 > Article
-
Original Article
Interaction between vitamin E intake and a COMT gene variant on colorectal cancer risk among Korean adults: a case-control study -
Shinyoung Jun1*
 , Madhawa Gunathilake1, Jeonghee Lee1, Jae Hwan Oh2, Hee Jin Chang2, Dae Kyung Sohn2, Aesun Shin3,4, Jeongseon Kim5
, Madhawa Gunathilake1, Jeonghee Lee1, Jae Hwan Oh2, Hee Jin Chang2, Dae Kyung Sohn2, Aesun Shin3,4, Jeongseon Kim5 -
Epidemiol Health 2023;45:e2023100.
DOI: https://doi.org/10.4178/epih.e2023100
Published online: November 14, 2023
1Department of Cancer Biomedical Science, National Cancer Center Graduate School of Cancer Science and Policy, Goyang, Korea
2Center for Colorectal Cancer, National Cancer Center, Goyang, Korea
3Department of Preventive Medicine, Seoul National University College of Medicine, Seoul, Korea
4Cancer Research Institute, Seoul National University, Seoul, Korea
5Department of Cancer, AI & Digital Health, National Cancer Center Graduate School of Cancer Science and Policy, Goyang, Korea
- Correspondence: Jeongseon Kim, Department of Cancer, AI & Digital Health, National Cancer Center Graduate School of Cancer Science and Policy, 323 Ilsan-ro, Ilsandong-gu, Goyang 10408, Korea, E-mail: jskim@ncc.re.kr
- * Current affiliation: Department of Food Science and Nutrition, Soonchunhyang University, Asan, Korea.
© 2023, Korean Society of Epidemiology
This is an open-access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,886 Views
- 103 Download
Abstract
-
OBJECTIVES
- Previous human trials have not supported the anticarcinogenic effect of vitamin E despite biological plausibility and considerable epidemiological evidence. A possible explanation for this inconsistency is the interactive effect of the catechol-O-methyltransferase (COMT) gene and supplemental vitamin E on cancer. We examined whether a COMT gene variant modulates the effect of dietary vitamin E intake on colorectal cancer (CRC) risk.
-
METHODS
- In this case-control study of Korean adults (975 cases and 975 age- and sex-matched controls), dietary vitamin E density (mg/1,000 kcal) was measured using a semiquantitative food frequency questionnaire, COMT single nucleotide polymorphism (SNP) rs740603 (A>G) was genotyped, and CRC was verified histologically. We estimated odds ratios (ORs) and 95% confidence intervals (CIs) using unconditional logistic regression models with adjustments for potential confounders.
-
RESULTS
- Higher vitamin E density was associated with a lower risk of CRC (highest vs. lowest quartiles: OR, 0.72; 95% CI, 0.55 to 0.96; p-for-trend=0.002). When stratified by COMT SNP rs740603 genotype, the inverse association between vitamin E density and CRC risk was confined to those with at least 1 A allele (≥median vs. <median: OR, 0.63; 95% CI, 0.51 to 0.78). The interaction between rs740603 and vitamin E density was significant (p-for-interaction=0.020). No direct association was observed between COMT SNP rs740603 and CRC risk (OR, 1.08; 95% CI, 0.83 to 1.41).
-
CONCLUSIONS
- Our findings support a role for a genetic polymorphism in COMT in modifying the association between dietary vitamin E intake and CRC.
- Due to its antioxidant properties, vitamin E has been expected to prevent cancer development [1]. Supporting this hypothesis, a considerable number of epidemiological studies have reported that higher vitamin E intake is associated with reduced risks of various cancer types [2–7]. However, randomized controlled trials that were designed to confirm those epidemiological findings have failed to confirm a role of vitamin E supplementation in cancer prevention [8].
- Recent results on gene-environment interactions offered a possible explanation for the inconsistent findings on vitamin E and cancer, suggesting that genetic variants involved in oxidant enzyme activity may have confounded the association between vitamin E and cancer risk [9]. In 2 large randomized controlled trials of vitamin E (alpha-tocopherol) supplementation in populations of European ancestry, polymorphisms in the catechol-O-methyltransferase (COMT) gene significantly modified the effect of vitamin E on total cancer incidence [9]. The interactive effects did not reach statistical significance when focusing on specific cancer types, but the pattern of vitamin E being beneficial only among rs4680 Met-allele homozygotes was generally consistent for breast cancer and colorectal cancer (CRC) [9]. Questions for further research included whether the pharmacogenetic effect of vitamin E and COMT on cancer prevention extends to dietary vitamin E intake and to specific cancer types.
- Therefore, we examined whether a polymorphism in COMT modulates the effect of dietary vitamin E intake on CRC risk in a case-control study of Korean adults. CRC is the third most common cancer both in Korea and worldwide, and effective and feasible prevention strategies are necessary [10]. We focused on the single-nucleotide polymorphism (SNP) rs740603 (A>G), which was shown to modify the effect of dietary vitamin E intake on waist circumference in a Spanish case-control study [11].
INTRODUCTION
- Study population
- CRC case-control data were collected at the National Cancer Center Korea. Case participants were recruited among patients who were newly diagnosed with adenocarcinoma of the colon or rectum based on endoscopic biopsies. There were 2 rounds of data collection: first, from August 2010 to August 2013; and second, from January 2018 to September 2020. Control participants were recruited from cancer-free individuals who came for a health checkup at the National Cancer Center Korea from October 2007 to December 2021 [12].
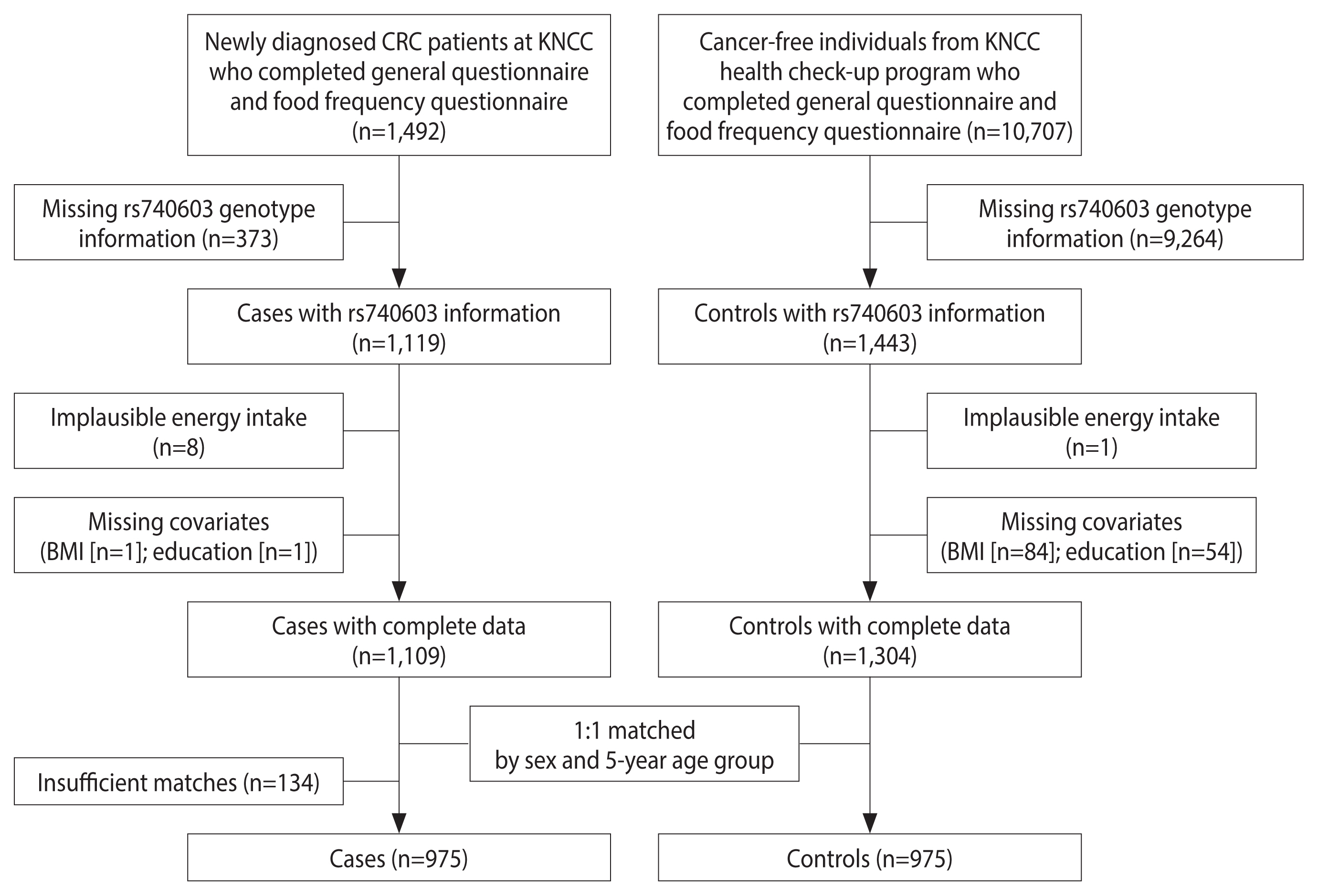
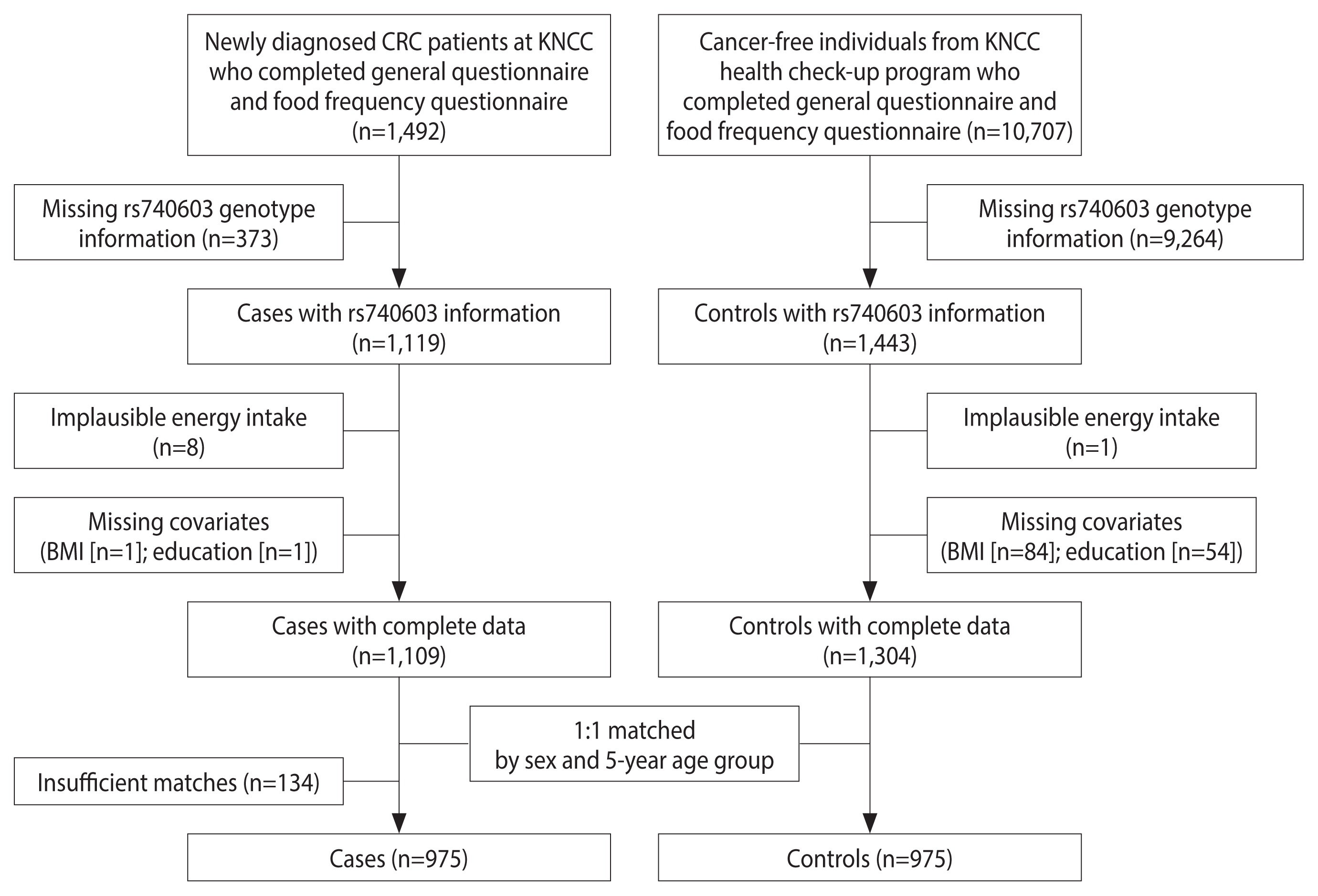
- The study participant selection process is described in Figure 1. From 1,492 cases and 10,707 controls who completed the general questionnaire and food frequency questionnaire (FFQ), we were able to successfully obtain rs740603 genotype information in 1,119 cases and 1,443 controls. We then excluded those with implausible energy intake (<500 or >4,000 kcal/day regardless of sex [13,14]; 8 cases and 1 control), missing body mass index (BMI) information (1 case and 84 controls), or missing education information (1 case and 54 controls). Among the remaining 1,109 cases and 1,304 controls, controls were matched to cases by sex and 5-year age group at a 1:1 ratio using a published macro [15]. As a result, 975 cases and 975 controls were matched successfully and were included in our analysis.
- Data collection
- Trained interviewers administered the general questionnaire on socio-demographic, lifestyle, and health characteristics and the 106-item semiquantitative FFQ. To minimize recall bias, we contacted cases within a few days after the first hospital admission and asked them to report their lifestyles and habitual diets before CRC diagnosis. The FFQ was developed to assess Korean adults’ diets and has been validated against 12-day dietary records across seasons [16]. Daily energy intake and vitamin E intake (i.e., sum of α-, β-, γ-, δ-tocopherols and α-, β-, γ-, δ-tocotrienols) were calculated using the Computer Aided Nutrition Analysis Program version 4 (Can-Pro 4.0; Korean Nutrition Society, Seoul, Korea). To adjust for energy and measurement errors associated with the FFQ [17], vitamin E density was calculated as the ratio of dietary vitamin E intake to total dietary energy intake (mg/1,000 kcal). Vitamin C density was calculated using the same method. We also calculated the Korea Healthy Eating Index, which represents overall dietary quality by measuring adherence to the Dietary Guidelines for Koreans [18].
- Anthropometric measurements and a blood draw were conducted by trained health technicians on the same day or within a few days of the administration of the questionnaire. BMI was calculated as weight in kilograms divided by the square of height in meters. Obesity was defined as BMI>25 kg/m2 based on the Asian-specific cut-off [19]. If height and body weight measurements were missing (567 cases and 376 controls), self-reported height and weight were used to calculate the BMI. Among 599 participants who had both measured and self-reported anthropometry data, the correlation coefficients between self-reported and measured height and weight were very high (≥0.98).
- Single-nucleotide polymorphism genotyping
- From blood samples, DNA was extracted using the MagAttract DNA Blood M48 Kit (Qiagen, Hilden, Germany) and the BioRobot M48 automatic extraction equipment (Qiagen). SNP genotyping was performed using the Illumina MEGA-Expanded Array (Illumina Inc., Hayward, CA, USA) consisting of 123K SNPs. To increase genome coverage, we imputed untyped SNPs, including rs740603, using the Michigan imputation server with the 1000 Genome Project phase 3 East Asian ancestry as a reference panel.
- Per a priori quality control criteria, we subsequently excluded (1) SNPs with a genotype call rate <98%, (2) individuals with a genotype call rate <98%, (3) SNPs with minor allele frequency (MAF) <5%, (4) SNPs with a Hardy-Weinberg equilibrium p-value <1×10−6, and (5) those related based on pairwise identity-by-decent proportion (pi-hat threshold of 0.25).
- Statistical analysis
- Descriptive statistics for cases and controls are presented as numbers (%) for categorical variables or means±standard deviations for continuous variables. The significance of differences between cases and controls was determined based on the chi-square test for categorical variables and the t-test for continuous variables.
- We used unconditional logistic regression models with adjustment for covariates selected based on the previous literature, biological plausibility, and collinearity to estimate odds ratios (ORs) and 95% confidence intervals (CIs) for the association between vitamin E density or the SNP rs740603 and CRC risk. Vitamin E density was divided into quartiles based on the distribution of controls, and the rs740603 genotype was combined based on a dominant model, with the A allele regarded as a dominant allele because the presence of the A allele was associated with a lower waist circumference and interacted with vitamin E intake [11]. We then examined diet-gene interactions by conducting logistic regression analyses stratified by the rs740603 genotype and assessing the statistical significance of the interaction by using the Wald test for cross-product terms of vitamin E density and the rs740603 genotype. Vitamin E density was divided into 2 groups (< and ≥ median based on the distribution in controls) to secure sufficient statistical power. Model 1 included matching factors (age and sex), total energy intake, and first-degree family history of CRC. Model 2 additionally included socioeconomic and lifestyle factors, such as smoking, drinking, education, and obesity.
- In sensitivity analyses, the rs740603 genotype was also tested in both recessive and codominant models (Supplementary Materials 1 and 2). Given the possible synergy between vitamins E and C [20], we also examined joint associations of vitamin E density (< and ≥ median based on the distribution in controls) and vitamin C density (< and ≥ median based on the distribution of controls) with CRC risk stratified by rs740603 genotype (Supplementary Material 3). We also tested the inclusion of the Korean Healthy Eating Index score in addition to all covariates in model 2, but did not present the results due to concerns about overadjustment bias.
- All analyses were conducted using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). All statistical tests were 2-sided and used a significance level of 0.05.
- Ethics statement
- This study was approved by the Institutional Review Board of the National Cancer Center Korea (No. NCC 2022-0118), and written informed consent was obtained from all study participants.
MATERIALS AND METHODS
- The general characteristics of the case participants and control participants are presented in Table 1. Compared with controls, cases were slightly younger, were less likely to have college degrees and be never-drinkers, and were more likely to have a first-degree family history of CRC. Cases had higher intakes of total energy and vitamin E but had a lower vitamin E density than controls. No significant differences in smoking, obesity, Korean Healthy Eating Index score, or rs740603 genotype between cases and controls were noted.
- We first examined the association between vitamin E density and the risk of CRC (Table 2). Statistically significant inverse associations between vitamin E density and CRC risk were observed when adjusted for age, sex, total energy intake, and first-degree family history of CRC without socioeconomic and lifestyle factors (model 1; Q4 vs. Q1: OR, 0.60; 95% CI, 0.46 to 0.78; p-for-trend <0.001) or with socioeconomic and lifestyle factors (model 2; Q4 vs. Q1: OR, 0.72; 95% CI, 0.55 to 0.96; p-for-trend=0.002).
- We also examined the relationship between COMT SNP rs740603 (G/G vs. A/A or A/G; dominant model) and the risk of CRC (Table 3). No significant association was observed (model 2; OR, 1.08; 95% CI, 0.83 to 1.41). No significant association was noted in either the recessive or codominant model (Supplementary Material 1).
- We then examined whether the association between vitamin E density and CRC risk varied according to the SNP rs740603 genotype (Table 4). The inverse association was confined to those with at least one A allele (model 2; p-for-interaction=0.02). Compared with lower vitamin E density (<median), higher vitamin E density (≥median) was associated with an OR of 0.63 (model 2; 95% CI, 0.51 to 0.78) among those with at least 1 A allele (A/A or A/G). Vitamin E density was not associated with CRC risk among those with the G/G genotype (model 2; OR, 1.13; 95% CI, 0.66 to 1.91). The results were consistent in the codominant model, with significant associations between vitamin E density and CRC risk only noted in those with A/A and A/G genotypes (Supplementary Material 2). In the recessive model, significant associations between vitamin E density and CRC risk were observed not only in those with the A/A genotype but also in those with the G/G or A/G genotype, which may have been driven by a significant association among those with the A/G genotype.
- In the joint analysis of vitamin C and vitamin E density, vitamin E largely drove the associations. Briefly, significant associations were observed only between the higher dietary vitamin E density group, with either lower or higher vitamin C density, and CRC risk among participants with at least 1 A allele (Supplementary Material 3).
RESULTS
- Despite biological plausibility [1] and considerable epidemiological evidence [6,21–23] suggesting that vitamin E plays a protective role in CRC development [8], human trials have not supported the anticarcinogenic effect of supplemental vitamin E. A possible explanation for this inconsistency is the interactive effect of COMT and supplemental vitamin E on cancer [9]. Our results suggest that the interaction observed among participants of European ancestry [9] may be applicable to dietary vitamin E and CRC among participants of Asian ethnicity. In our study of Korean adults, dietary vitamin E intake was protective against CRC development only in carriers of the COMT rs740603 A allele, but not in those who were homozygotes for the G allele.
- The enzyme encoded by COMT catalyzes the O-methylation of various compounds, including catecholamines, catechol estrogens, and dietary polyphenols. Therefore, the COMT enzyme has been implicated in multiple neuropsychiatric disorders [24,25] and metabolic disorders [11,26–28]. However, insignificant associations have been reported between COMT and CRC incidence and survival [29,30], suggesting that COMT might interact with environmental factors in modulating carcinogenesis. Indeed, in our study, COMT rs740603 was not directly associated with CRC, but rather modified the association between dietary vitamin E and CRC risk. The SNP rs740603 is located within intron 1 and is approximately 6.1 kb 5’ to rs4680, the most studied functional variant. This polymorphism was identified as a potentially functional variant associated with a psychiatric phenotype [31] and had interactive effects with dietary vitamin E intake on waist circumference [11]. We were unable to examine whether rs4680 has similar effects to those of rs740603 due to a lack of genotype data, but a weak correlation has been found between rs4680 and rs740603 in East Asian populations (1000 Genomes; R2=0.11) [32]. Future studies could investigate whether rs4680 or other variants correlated with rs740603 may be involved in the interaction between rs740603 and dietary vitamin E on CRC.
- The mechanisms underlying this interaction between vitamin E and COMT need further investigation, but the interaction may be related to oxidative stress management based on the following data. The knockdown of COMT expression was shown to increase estradiol-induced or catechol estrogen-induced reactive oxygen species, microsatellite instability, and neoplastic transformation of endometrial glandular cells [33]. In platelets, the COMT enzyme was shown to methylate quercetin, which is an antioxidant [34]. A recent report on the interactive effect of polymorphisms of IL-10 and COMT may have implications regarding the potential interplay between the dopaminergic system and the inflammatory system [35]. However, the possible role of vitamin C in this interaction proposed by a previous study [9] based on its association with the COMT gene [36], as well as its synergistic interaction with vitamin E [20], was not supported in our study, suggesting that vitamin E may be involved in a unique mechanism.
- In the absence of stratification by rs740603, we observed that dietary vitamin E intake was inversely associated with CRC risk, which is consistent with many previous epidemiological studies [6,21–23]. Because the G allele is a minor allele in the Asian population (MAF of 0.41 in this study sample and 0.40 in the East Asian population from 1000 Genomes), null associations in G allele homozygotes seem diluted when all rs740603 genotypes are combined. Regarding the null findings from previous human trials [8] and some epidemiological studies [37,38], we speculate that the composition (only alpha-tocopherol) and high dose of supplemental vitamin E provided in the trial [1] or the large variation in linkage disequilibrium patterns across populations (especially between European and East Asian populations) [39] may have affected the results.
- Our data should be understood within the context of the study’s strengths and limitations. The strengths of our study include histological verification of CRC patients and the use of a validated FFQ. In addition, we adjusted for a range of plausible confounders measured by a comprehensive questionnaire and clinical assessments, although there is always a possibility of residual confounding.
- One of the major limitations of this study was the absence of other populations to test the replicability of our results. Moreover, the case-control study design employed in our study is susceptible to recall bias and selection bias. To minimize recall bias, we interviewed CRC patients immediately after hospital admission for surgery and asked them to report their habitual diet and lifestyle prior to diagnosis. To minimize selection bias, we selected control participants from those who visited the same hospital for health check-ups supported by the Korea National Screening Program; however, the control participants who voluntarily came for check-ups may have been more health-conscious than the case participants. Another major limitation is the lack of supplemental vitamin E intake information. As dietary supplements are used by approximately 25% of Korean adults [40], we suggest that future investigations should be conducted with complete information on dietary and supplemental vitamin E information to confirm our findings. Of note, our vitamin E estimate was a simple sum of four tocopherols (α, β, γ, δ) and four tocotrienols (α, β, γ, δ) in milligrams per day. Future studies may also explore the different chemical forms of vitamin E given the growing attention on the anticarcinogenic effects of γ- and δ-tocopherols [41].
- In conclusion, the COMT genetic variant modified the association between dietary vitamin E intake and CRC; specifically, vitamin E was inversely associated with CRC risk only in carriers of the COMT rs740603 A allele. These findings add key evidence to the literature on nutrient-gene interactions affecting CRC risk and may inform future precision nutrition research and practice in cancer prevention.
DISCUSSION
DATA AVAILABILITY
SUPPLEMENTARY MATERIALS
-
CONFLICT OF INTEREST
The authors have no conflicts of interest to declare for this study.
-
FUNDING
This work was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (2021R1A6A3A01087058) and by the NRF grant funded by the Ministry of Science and ICT (2021R1A2C2008439).
-
AUTHOR CONTRIBUTIONS
Conceptualization: Jun S. Data curation: Lee J, Oh JH, Chang HJ, Sohn DK, Shin A, Kim J. Funding acquisition: Jun S, Kim J. Methodology: Jun S, Gunathilake M. Project administration: Lee J. Visualization: Jun S. Writing – original draft: Jun S. Writing – review & editing: Gunathilake M, Lee J, Oh JH, Chang HJ, Sohn DK, Shin A, Kim J.
NOTES
ACKNOWLEDGEMENTS
| Characteristics | Cases (n=975) | Controls (n=975) | p-value1 |
|---|---|---|---|
| Age (yr) | 56.3±8.9 | 57.2±8.8 | 0.015 |
| Sex | >0.999 | ||
| Male | 605 (62.1) | 605 (62.1) | |
| Female | 370 (38.0) | 370 (38.0) | |
| Education | <0.001 | ||
| Less than high school | 300 (30.8) | 123 (12.6) | |
| High school graduate or associate’s degree | 411 (42.2) | 415 (42.6) | |
| College graduate or more | 264 (27.1) | 437 (44.8) | |
| Smoking | 0.368 | ||
| Current | 481 (49.3) | 457 (46.9) | |
| Past | 344 (35.3) | 347 (35.6) | |
| Never | 150 (15.4) | 171 (17.5) | |
| Drinking | |||
| Current | 370 (38.0) | 295 (30.3) | <0.001 |
| Past | 146 (15.0) | 94 (9.6) | |
| Never | 459 (47.1) | 586 (60.1) | |
| Obesity (BMI>25 kg/m2) | 352 (36.1) | 339 (34.8) | 0.538 |
| First-degree family history of colorectal cancer | 91 (9.3) | 62 (6.4) | 0.015 |
| Total energy intake (kcal/day) | 1,938.0±558.7 | 1,648.0±564.1 | <0.001 |
| Vitamin E intake (mg/day) | 9.6±4.1 | 8.6±4.1 | <0.001 |
| Vitamin E density (mg/1,000 kcal) | 4.9±1.3 | 5.2±1.5 | <0.001 |
| Korean Healthy Eating Index | 58.1±9.2 | 58.8±10.8 | 0.150 |
| rs740603 genotype | 0.998 | ||
| A/A | 336 (34.5) | 336 (34.5) | |
| A/G | 483 (49.5) | 482 (49.4) | |
| G/G | 156 (16.0) | 157 (16.1) |
| Vitamin E density (mg/1,000 kcal) | No. of cases/controls | Model 11 | Model 22 |
|---|---|---|---|
| Q1 (≤4.16) | 308/243 | 1.00 (reference) | 1.00 (reference) |
| Q2 (>4.16 and ≤5.03) | 279/244 | 0.78 (0.61, 0.999) | 0.84 (0.64, 1.09) |
| Q3 (>5.03 and ≤5.93) | 176/244 | 0.47 (0.36, 0.62) | 0.55 (0.41, 0.73) |
| Q4 (>5.93) | 212/244 | 0.60 (0.46, 0.78) | 0.72 (0.55, 0.96) |
| p-for-linear trend | <0.001 | 0.002 |
| COMT SNP rs7406031 | No. of cases/controls | Model 12 | Model 23 |
|---|---|---|---|
| G/G | 156/157 | 1.00 (reference) | 1.00 (reference) |
| A/A+A/G | 819/818 | 1.07 (0.84, 1.38) | 1.08 (0.83, 1.41) |
Values are presented as odds ratio (95% confidence interval).
CRC, colorectal cancer; COMT, catechol-O-methyltransferase; SNP, single-nucleotide polymorphism.
1 Dominant model.
2 Adjusted for age, sex, total energy intake and first-degree family history of CRC.
3 Adjusted for age, sex, total energy intake, first-degree family history of CRC, smoking, drinking, education, and obesity.
| COMT SNP rs7406031 | Lower vitamin E2 | Higher vitamin E2 | p-value |
|---|---|---|---|
| G/G | |||
| No. of cases/controls | 89/89 | 67/68 | |
| Model 13 | 1.00 (reference) | 0.88 (0.54, 1.43) | 0.611 |
| Model 24 | 1.00 (reference) | 1.13 (0.66, 1.91) | 0.662 |
| A/A+A/G | |||
| No. of cases/controls | 498/398 | 321/420 | |
| Model 13 | 1.00 (reference) | 0.56 (0.46, 0.69) | <0.001 |
| Model 24 | 1.00 (reference) | 0.63 (0.51, 0.78) | <0.001 |
Values are presented as odds ratio (95% confidence interval).
CRC, colorectal cancer; COMT, catechol-O-methyltransferase; SNP, single-nucleotide polymorphism.
1 Dominant model.
2 Lower and higher vitamin E groups had vitamin E density at or below and above the median (5.03 mg/1,000 kcal), respectively.
3 Adjusted for age, sex, total energy intake and first-degree family history of CRC; p-for-interaction=0.060.
4 Adjusted for age, sex, total energy intake, first-degree family history of CRC, smoking, drinking, education, and obesity; p-for-interaction=0.020.
- 1. Jiang Q. Natural forms of vitamin E and metabolites-regulation of cancer cell death and underlying mechanisms. IUBMB Life 2019;71:495-506.ArticlePubMedPDF
- 2. Stolzenberg-Solomon RZ, Sheffler-Collins S, Weinstein S, Garabrant DH, Mannisto S, Taylor P, et al. Vitamin E intake, alpha-tocopherol status, and pancreatic cancer in a cohort of male smokers. Am J Clin Nutr 2009;89:584-591.PubMed
- 3. Huang J, Weinstein SJ, Yu K, Männistö S, Albanes D. A prospective study of serum vitamin E and 28-year risk of lung cancer. J Natl Cancer Inst 2020;112:191-199.ArticlePubMedPMCPDF
- 4. Lawrence WR, Lim JE, Huang J, Weinstein SJ, Männistö S, Albanes D. A 28-year prospective analysis of serum vitamin E, vitamin E-related genetic variation and risk of prostate cancer. Prostate Cancer Prostatic Dis 2022;25:553-560.ArticlePubMedPMCPDF
- 5. Nagel G, Linseisen J, van Gils CH, Peeters PH, Boutron-Ruault MC, Clavel-Chapelon F, et al. Dietary beta-carotene, vitamin C and E intake and breast cancer risk in the European Prospective Investigation into Cancer and Nutrition (EPIC). Breast Cancer Res Treat 2010;119:753-765.ArticlePubMedPDF
- 6. Park Y, Spiegelman D, Hunter DJ, Albanes D, Bergkvist L, Buring JE, et al. Intakes of vitamins A, C, and E and use of multiple vitamin supplements and risk of colon cancer: a pooled analysis of prospective cohort studies. Cancer Causes Control 2010;21:1745-1757.ArticlePubMedPMCPDF
- 7. Egnell M, Fassier P, Lécuyer L, Gonzalez R, Zelek L, Vasson MP, et al. Antioxidant intake from diet and supplements and risk of digestive cancers in middle-aged adults: results from the prospective NutriNet-Santé cohort. Br J Nutr 2017;118:541-549.ArticlePubMed
- 8. O’Connor EA, Evans CV, Ivlev I, Rushkin MC, Thomas RG, Martin A, et al. Vitamin and mineral supplements for the primary prevention of cardiovascular disease and cancer: updated evidence report and systematic review for the US Preventive Services Task Force. JAMA 2022;327:2334-2347.ArticlePubMed
- 9. Hall KT, Buring JE, Mukamal KJ, Vinayaga Moorthy M, Wayne PM, Kaptchuk TJ, et al. COMT and alpha-tocopherol effects in cancer prevention: gene-supplement interactions in two randomized clinical trials. J Natl Cancer Inst 2019;111:684-694.ArticlePubMedPMC
- 10. Kang MJ, Won YJ, Lee JJ, Jung KW, Kim HJ, Kong HJ, et al. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2019. Cancer Res Treat 2022;54:330-344.ArticlePubMedPMCPDF
- 11. Mansego ML, De Marco G, Ivorra C, Lopez-Izquierdo R, Morcillo S, Rojo-Martínez G, et al. The nutrigenetic influence of the interaction between dietary vitamin E and TXN and COMT gene polymorphisms on waist circumference: a case control study. J Transl Med 2015;13:286.ArticlePubMedPMC
- 12. Kim J. Cancer screenee cohort study of the National Cancer Center in South Korea. Epidemiol Health 2014;36:e2014013.ArticlePubMedPMC
- 13. Willett W. Nutritional epidemiology. 3rd ed. Oxford: Oxford University Press; 2013. p 260-286.
- 14. Santos DA, Silva AM, Matias CN, Magalhães JP, Fields DA, Minderico CS, et al. Validity of a combined heart rate and motion sensor for the measurement of free-living energy expenditure in very active individuals. J Sci Med Sport 2014;17:387-393.ArticlePubMed
- 15. Mortensen LQ, Andresen K, Burcharth J, Pommergaard HC, Rosenberg J. Matching cases and controls using SAS® software. Font Big Data 2019;2:4.ArticlePubMedPMC
- 16. Ahn Y, Kwon E, Shim JE, Park MK, Joo Y, Kimm K, et al. Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur J Clin Nutr 2007;61:1435-1441.ArticlePubMedPDF
- 17. Freedman LS, Commins JM, Moler JE, Willett W, Tinker LF, Subar AF, et al. Pooled results from 5 validation studies of dietary self-report instruments using recovery biomarkers for potassium and sodium intake. Am J Epidemiol 2015;181:473-487.ArticlePubMedPMC
- 18. Yun S, Park S, Yook SM, Kim K, Shim JE, Hwang JY, et al. Development of the Korean Healthy Eating Index for adults, based on the Korea National Health and Nutrition Examination Survey. Nutr Res Pract 2022;16:233-247.ArticlePubMedPMCPDF
- 19. Seo MH, Lee WY, Kim SS, Kang JH, Kang JH, Kim KK, et al. 2018 Korean Society for the Study of Obesity guideline for the management of obesity in Korea. J Obes Metab Syndr 2019;28:40-45.PubMedPMC
- 20. Niki E. Interaction of ascorbate and alpha-tocopherol. Ann N Y Acad Sci 1987;498:186-199.PubMed
- 21. Leenders M, Leufkens AM, Siersema PD, van Duijnhoven FJ, Vrieling A, Hulshof PJ, et al. Plasma and dietary carotenoids and vitamins A, C and E and risk of colon and rectal cancer in the European Prospective Investigation into Cancer and Nutrition. Int J Cancer 2014;135:2930-2939.ArticlePubMed
- 22. Luo H, Fang YJ, Lu MS, Pan ZZ, Huang J, Chen YM, et al. Dietary and serum vitamins A and E and colorectal cancer risk in Chinese population: a case-control study. Eur J Cancer Prev 2019;28:268-277.ArticlePubMed
- 23. Alves Ribeiro RR, Rolim de Brito I, Andrade Souza K, de Castro Souza L, Almeida de Oliveira T, Weller M. Risk of colorectal cancer in a Brazilian population is differentially associated with the intake of processed meat and vitamin E. Nutr Cancer 2022;74:820-829.ArticlePubMed
- 24. Pap D, Gonda X, Molnar E, Lazary J, Benko A, Downey D, et al. Genetic variants in the catechol-o-methyltransferase gene are associated with impulsivity and executive function: relevance for major depression. Am J Med Genet B Neuropsychiatr Genet 2012;159B:928-940.ArticlePubMed
- 25. Fiocco AJ, Lindquist K, Ferrell R, Li R, Simonsick EM, Nalls M, et al. COMT genotype and cognitive function: an 8-year longitudinal study in white and black elders. Neurology 2010;74:1296-1302.ArticlePubMedPMC
- 26. Htun NC, Miyaki K, Song Y, Ikeda S, Shimbo T, Muramatsu M. Association of the catechol-O-methyl transferase gene Val158Met polymorphism with blood pressure and prevalence of hypertension: interaction with dietary energy intake. Am J Hypertens 2011;24:1022-1026.ArticlePubMed
- 27. Voutilainen S, Tuomainen TP, Korhonen M, Mursu J, Virtanen JK, Happonen P, et al. Functional COMT Val158Met polymorphism, risk of acute coronary events and serum homocysteine: the Kuopio ischaemic heart disease risk factor study. PLoS One 2007;2:e181.ArticlePubMedPMC
- 28. Hall KT, Nelson CP, Davis RB, Buring JE, Kirsch I, Mittleman MA, et al. Polymorphisms in catechol-O-methyltransferase modify treatment effects of aspirin on risk of cardiovascular disease. Arterioscler Thromb Vasc Biol 2014;34:2160-2167.ArticlePubMedPMC
- 29. Landi S, Gemignani F, Moreno V, Gioia-Patricola L, Chabrier A, Guino E, et al. A comprehensive analysis of phase I and phase II metabolism gene polymorphisms and risk of colorectal cancer. Pharmacogenet Genomics 2005;15:535-546.ArticlePubMed
- 30. Passarelli MN, Newcomb PA, Makar KW, Burnett-Hartman AN, Phipps AI, David SP, et al. No association between germline variation in catechol-O-methyltransferase and colorectal cancer survival in postmenopausal women. Menopause 2014;21:415-420.ArticlePubMedPMC
- 31. Ittiwut R, Listman JB, Ittiwut C, Cubells JF, Weiss RD, Brady K, et al. Association between polymorphisms in catechol-O-methyltransferase (COMT) and cocaine-induced paranoia in European-American and African-American populations. Am J Med Genet B Neuropsychiatr Genet 2011;156B:651-660.ArticlePubMedPMC
- 32. Alexander TA, Machiela MJ. LDpop: an interactive online tool to calculate and visualize geographic LD patterns. BMC Bioinformatics 2020;21:14.ArticlePubMedPMCPDF
- 33. Salama SA, Kamel M, Awad M, Nasser AH, Al-Hendy A, Botting S, et al. Catecholestrogens induce oxidative stress and malignant transformation in human endometrial glandular cells: protective effect of catechol-O-methyltransferase. Int J Cancer 2008;123:1246-1254.ArticlePubMed
- 34. Wright B, Gibson T, Spencer J, Lovegrove JA, Gibbins JM. Platelet-mediated metabolism of the common dietary flavonoid, quercetin. PLoS One 2010;5:e9673.ArticlePubMedPMC
- 35. Wang J, Xu H, Wang D, Wei G, Zhou H, Wang L, et al. The interactive effect of genetic polymorphisms of IL-10 and COMT on cognitive function in schizophrenia. J Psychiatr Res 2021;136:501-507.ArticlePubMed
- 36. Shin SY, Fauman EB, Petersen AK, Krumsiek J, Santos R, Huang J, et al. An atlas of genetic influences on human blood metabolites. Nat Genet 2014;46:543-550.ArticlePubMedPMCPDF
- 37. Wang Z, Joshi AM, Ohnaka K, Morita M, Toyomura K, Kono S, et al. Dietary intakes of retinol, carotenes, vitamin C, and vitamin E and colorectal cancer risk: the Fukuoka colorectal cancer study. Nutr Cancer 2012;64:798-805.ArticlePubMed
- 38. Heine-Bröring RC, Winkels RM, Renkema JM, Kragt L, van Orten-Luiten AC, Tigchelaar EF, et al. Dietary supplement use and colorectal cancer risk: a systematic review and meta-analyses of prospective cohort studies. Int J Cancer 2015;136:2388-2401.ArticlePubMed
- 39. Mukherjee N, Kidd KK, Pakstis AJ, Speed WC, Li H, Tarnok Z, et al. The complex global pattern of genetic variation and linkage disequilibrium at catechol-O-methyltransferase. Mol Psychiatry 2010;15:216-225.ArticlePubMedPMCPDF
- 40. Kim S, Song Y, Lee JE, Jun S, Shin S, Wie GA, et al. Total antioxidant capacity from dietary supplement decreases the likelihood of having metabolic syndrome in Korean adults. Nutrients 2017;9:1055.ArticlePubMedPMC
- 41. Yang CS, Luo P, Zeng Z, Wang H, Malafa M, Suh N. Vitamin E and cancer prevention: studies with different forms of tocopherols and tocotrienols. Mol Carcinog 2020;59:365-389.ArticlePubMedPMCPDF
 PubReader
PubReader ePub Link
ePub Link Cite
Cite